Location: Home >> Detail
J Psychiatry Brain Sci. 2025;10(4):e250008. https://doi.org/10.20900/jpbs.20250008
 ,
Sarah Nash 1 ,
Anne Sadler 2,3 ,
Emily Roberts 4 ,
James Torner 1 ,
Jonathan Platt 1
,
Sarah Nash 1 ,
Anne Sadler 2,3 ,
Emily Roberts 4 ,
James Torner 1 ,
Jonathan Platt 1
1 Department of Epidemiology, College of Public Health, University of Iowa, Iowa City, IA 52242, USA
2 Department of Psychiatry, Carver College of Medicine, University of Iowa, Iowa City, IA 52242, USA
3 Center for Access and Delivery Research and Evaluation, Iowa City VA Health Care System, Iowa City, IA 52246, USA
4 Department of Biostatistics, College of Public Health, University of Iowa, Iowa City, IA 52242, USA
* Correspondence: Amanda Sursely
This article belongs to the Virtual Special Issue "JPBS 10th Anniversary Special Issue"
Objective: Precipitating circumstances are life events that occur prior to suicide death. These events elevate risk through their interactions with individual characteristics, environmental factors, and internal processes. Thus, the influence of any one event on suicide requires understanding the social context within which it occurs. This study aimed to identify contextual patterns of precipitating circumstances using suicide narrative reports.
Methods: The National Violent Death Reporting System (NVDRS) is a surveillance system that aggregates data from all violence-related fatalities in the US, including suicide. This dataset includes a qualitative narrative for each case with in-depth information about the circumstances surrounding the death. For each circumstance, 100 randomly selected narrative reports were reviewed and coded via inductive summative content analysis.
Results: A total of 1670 narrative reports were analyzed, across 17 distinct circumstance categories. For each circumstance, contextual factors causing, surrounding, and stemming from the circumstance were identified. For example, the circumstance “financial crisis” was often caused by a recent job loss, chronic unemployment, substance use, or a medical condition. This crisis manifested as either general financial stress, accumulated debt, or a failing business. As a result of the financial crisis, individuals experienced housing issues, interpersonal conflict, compromised medical care, bankruptcy, and a loss of material goods.
Conclusion: This study highlights that rarely does a single crisis elevate suicide risk, but rather each death reflects a web of related circumstances and their compounding effects. Recognizing these interconnected factors is essential for developing more comprehensive prevention strategies that address multiple, overlapping stressors rather than focusing on isolated risk factors.
Suicidal behavior exists along a continuum, encompassing suicidal ideation, suicide attempt, and death by suicide. The psychology of suicide is complex and multifaceted, but research has consistently linked negative life events (hereafter referred to as precipitating circumstances [1,2]), such as financial strain or interpersonal conflict, to heightened risk of suicide death [1,3,4]. Theoretical frameworks such as Joiner’s Interpersonal Theory of Suicide (IPTS) and the Integrated Motivational–Volitional (IMV) Model of Suicidal Behavior offer insight into how precipitating circumstances may contribute to suicidal behavior [5,6]. These models suggest that suicidal ideation arises from internal experiences such as perceived burdensomeness and thwarted belongingness, while the transition from suicidal ideation to action occurs when individuals acquire the capability to act, often facilitated by acute exposure to precipitating circumstances.
When studying precipitating circumstances, researchers commonly use broad categories (e.g., “interpersonal problems” or “physical health problems”) that span long timeframes across the life course. While informative, these labels and timeframes lack the temporal and contextual specificity needed to understand the acute crises that immediately precede suicide deaths. Crisis events, often unfolding over days or weeks prior to death, may be particularly important for identifying windows of opportunity for intervention [7], yet little is known about the specific events that constitute them. For example, it is unclear what specific events or experiences fall under the umbrella of an ‘interpersonal crisis’ or a ‘criminal crisis’ related to a suicide death. In addition, whilst precipitating circumstances are each individually associated with increased risk of suicide death, suicide is not a simple psychological problem that can be explained by the presence or absence of a single risk factor alone. Rather, it is inextricably shaped by the individual, social and cultural contexts in which it occurs [8]. Thus, the influence of any one precipitating factor on suicide requires a deeper understanding of the context in which it occurs. To gain a more detailed understanding of how precipitating circumstances influence suicide death it is crucial to explore the individual stories comprising the broad categories, examining how specific precipitating events unfold in real-world cases.
In this study, we utilized narrative data from the NVDRS to qualitatively examine the contextual details underlying each category of precipitating circumstance. We focused on three specific research questions (1) What specific experiences constitute each broad category of precipitating circumstance? (2) What additional context is needed to understand the circumstances? (3) How are the circumstances related to one another? We aimed to uncover details and relationships that are crucial for understanding how precipitating circumstances drive suicidal behavior in real-world cases.
The NVDRS is a case-only state-based surveillance system that aggregates data from all homicide, suicide, and legal intervention deaths in the US [9]. The complete details of this dataset are provided elsewhere [10]. For each case, it is recorded if each of 17 precipitating circumstances were present/absent prior to the death. For each present circumstance, it is further indicated whether this circumstance was a crisis, defined as occurring within the two weeks surrounding the death. Additionally, a qualitative incident narrative is provided describing the circumstances surrounding each death. The incident narratives are short reports compiled using coroner/medical examiner and law enforcement reports, suicide notes, and interviews with the decedents’ family/friends. These narrative reports contain a more detailed explanation of the circumstances surrounding each death that may not be captured in the categorical data [10].
Study PopulationThe initial population for this study consisted of all individuals aged 18–65 years who died by suicide between January 2012, and December 2021, as recorded in the NVDRS (n = 211,132). From this population, individuals for whom the circumstances surrounding their death were entirely unknown, there was no narrative data available, or who died in a murder-suicide were excluded (n = 130,338). Next, the population was further narrowed to exclude individuals who had experienced no circumstantial events within the two weeks prior to their death (n = 55,833). The final eligible population included 24,916 individuals.
Case SelectionFor each of the 17 precipitating circumstances in the NVDRS, we randomly selected 100 narratives wherein that circumstance was indicated to be present at the time of the death. If a circumstance had less than 100 narratives available, all were analyzed. This was done without replacement, such if a narrative had been analyzed for one circumstance, it could not then be selected for another. A sample size of 100 narratives was chosen as guided by the concept of information power [11] given the broad study question, the specificity of the experiences within each crisis category, the brevity of the narrative reports, and the cross-case analysis.
Narrative CodingNarrative data was analyzed via inductive summative content analysis [12]. Throughout the coding process, narratives were constantly analyzed and reanalyzed as new codes and themes emerged. A single researcher (AS) was responsible for the initial coding and re-coding for this project. After the completion of the initial codebook using a subset of narratives, two additional researchers (JP, SN) reviewed and provided feedback on how to better elicit the results and findings. Codes were iteratively categorized, sorted, added, deleted and redefined as necessary. AS then coded the interview transcripts, and re-presented results to the entire study team. The team reviewed the final codeset, and corresponding quotations to ensure coding accuracy. All discrepancies in coding were discussed amongst the team until consensus was reached. The narratives were coded in a circumstance-centered manner, such that only information pertaining to the current circumstance of interest was recorded. This was done to keep the focus on the events in the acute period surrounding the death. Importantly, only information explicitly stated in the narrative was recorded, inferences were not made (e.g., if a narrative stated that the decedent had lost their job, and was experiencing financial issues, the financial issues were not recorded as an effect of the job loss unless this was explicitly stated). All coding was completed using MaxQDA.
Reporting ConsiderationsThe goal of this research was to explore the specific experiences underlying each broad category of precipitating circumstance. Thus, the findings are presented in a manner that highlights the relative significance of each event, whilst also avoiding over-quantification by refraining from reporting exact case counts for each circumstance. The results are organized as follows: events were considered “very common” if they were present in more >50% of analyzed narratives, “somewhat common” if they were present in between 25–50% of analyzed narratives, “somewhat rare” if they were present in 10–25% of narratives, and “rare” if they were only found in less than 10% of narratives.
A total of 1670 narratives were analyzed. The demographic characteristics of the decedents included in this selected sample are presented in Table 1. Results were grouped into five domains based on their shared characteristics and themes, and included (1) addiction-related crises, (2) economic-related crises, (3) court-related crises, (4) relationship-related crises, and (5) other crises. For brevity, one example is presented for each domain, and the remainder can be found in Table 2, as well as in detail in Supplementary Material Tables S1–S5.
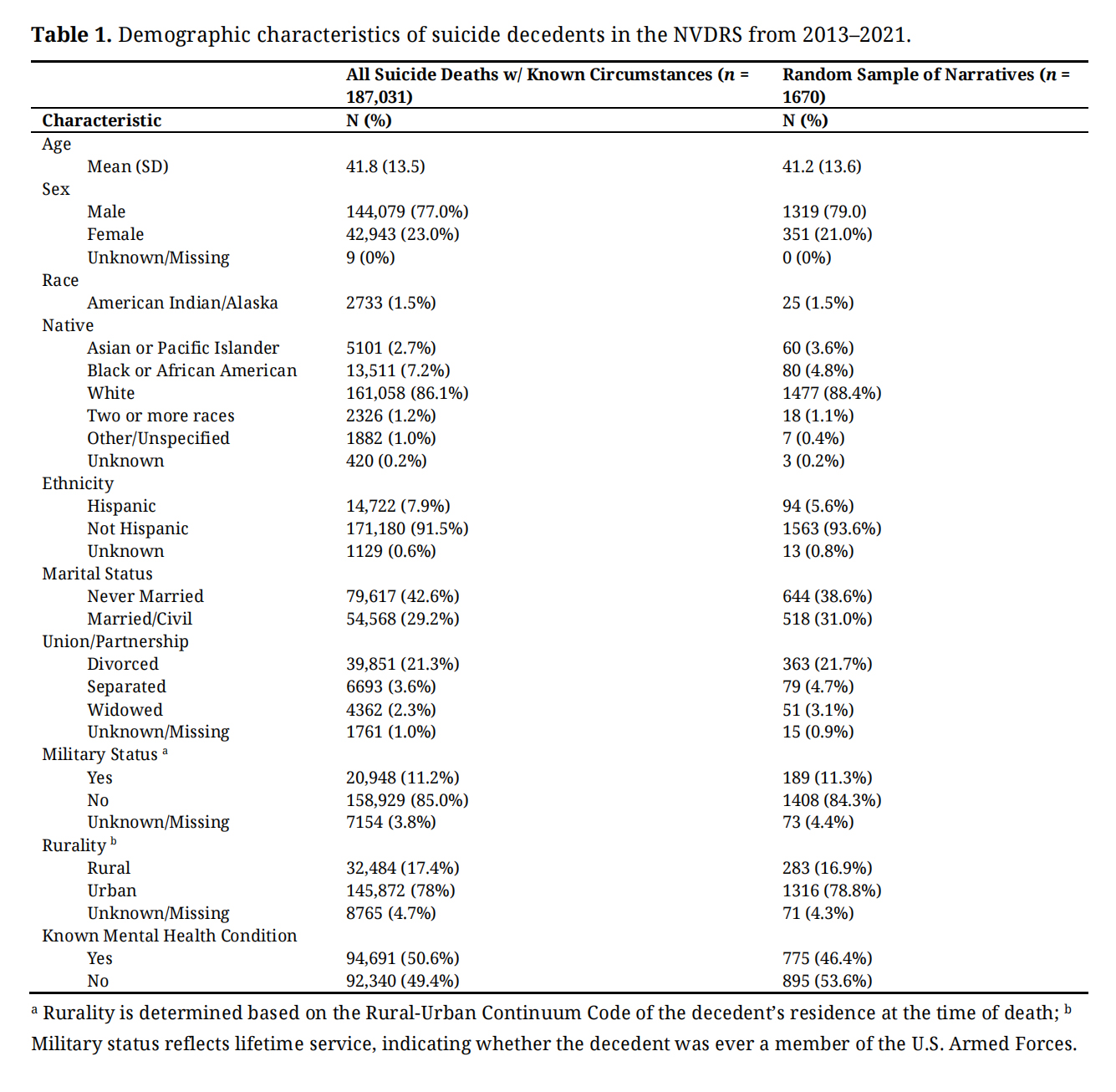 Table 1. Demographic characteristics of suicide decedents in the NVDRS from 2013–2021.
Table 1. Demographic characteristics of suicide decedents in the NVDRS from 2013–2021.
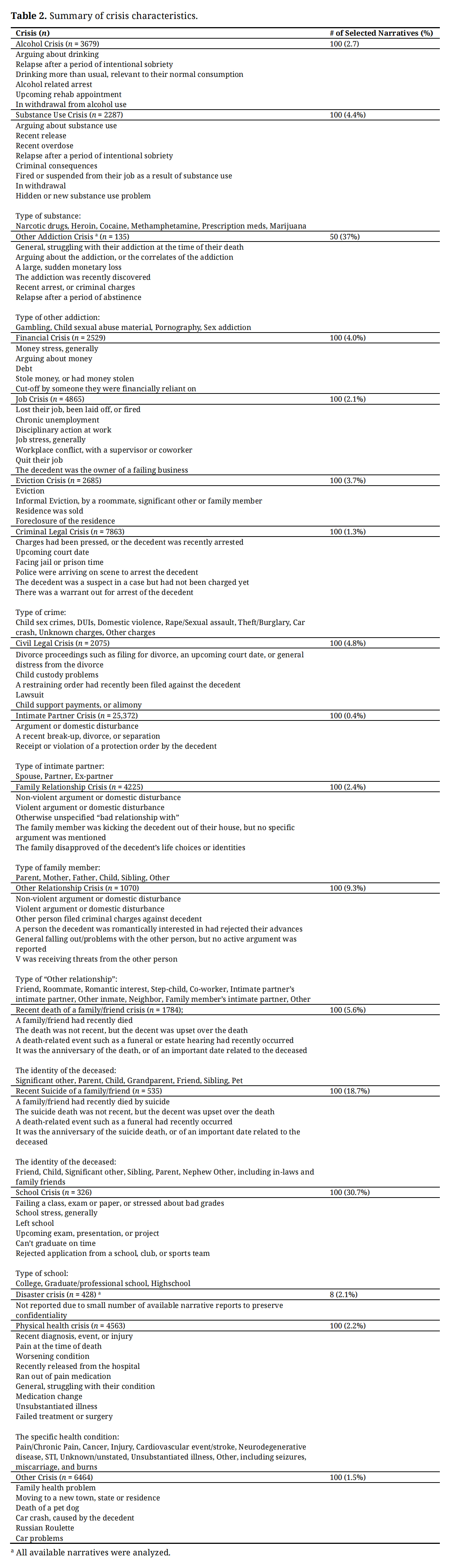 Table 2. Summary of crisis characteristics.
Table 2. Summary of crisis characteristics.
Addiction-related crises are summarized in detail in Supplementary Material Table S1. The three crisis types included in this domain included “Alcohol crisis”, “Substance use crisis” and “Other addiction crisis”. “Other addictions” were found to include addictions related to gambling, child sexual abuse material, pornography, and sex.
Alcohol CrisisVery common: It was very common for decedents to have a recorded history of alcohol abuse or alcohol use disorder.
Somewhat common: Arguments were somewhat common among decedents experiencing alcohol-related crises. These arguments often centered around the decedent’s drinking, level of intoxication, or alcohol misuse. In most cases, the arguments occurred with an intimate partner, such as a spouse or significant other.
Somewhat rare: It was somewhat rare for the decedent to have recently relapsed in the timeframe leading up to their death. This category also included cases where the decedent had significantly increased their alcohol consumption near the time of death, as well as instances where they had been arrested for alcohol-related offenses, such as a DUI or public intoxication. Some narratives indicated that the decedent became aggressive or perpetrated domestic violence due to the alcohol crisis. Other cases described the decedent being kicked out of their residence or facing eviction as a result of their alcohol-related struggles.
Rare: In rare instances, decedents were noted to be experiencing alcohol withdrawal at the time of their death or were preparing to check into a rehabilitation facility for alcohol use. A small number of cases documented a history of multiple DUI offenses or described decedents as being known to express suicidal thoughts while drinking.
Economic-Related CrisesEconomic-related crises are summarized in detail in Supplementary Material Table S2. The three crisis categories in this domain included “Financial crisis”, “Job crisis” and “Eviction crisis”.
Eviction CrisisSomewhat common: Formal eviction was somewhat common, typically caused by financial issues, job problems, or interpersonal conflicts.
Somewhat rare: Some narratives described decedents facing informal eviction from their residence, often at the request of roommate, significant other, or family member. These situations were sometimes attributed to interpersonal problems or substance use.
Rare: In rare instances, eviction crises were tied to the sale or foreclosure of the location where the decedent was residing.
Court-Related CrisesCourt-related crises are summarized in detail in Supplementary Material Table S3. The two crises in this domain include “Criminal legal crises” and “Civil legal crises”.
Criminal-Legal CrisisSomewhat common: Narratives frequently reported that the decedent had died following a recent arrest or after receiving criminal charges.
Somewhat rare: Child sex crimes, DUIs, and domestic violence cases were the most commonly mentioned offenses. In some cases, the decedent died in the days leading up to a scheduled court date or while facing significant jail or prison time as a result of their charges. There were also instances where the police were actively on the scene at the time of the decedent’s death, either to arrest them, question them, or serve a warrant.
Rare: In rare instances, the decedent was a suspect in a case but had not yet been charged, or there was an active warrant for their arrest. A few narratives described criminal issues leading to job loss or the filing of a restraining order against the decedent.
Relationship-Related CrisesRelationship-related crises are summarized in detail in Supplementary Material Table S4. The five crises in this domain include “Intimate Partner Crisis” ,“Family Relationship Crisis”, “Other Relationship Crisis”, “Death of a Family/Friend”, and “Suicide of a Family/Friend”.
Other Relationship CrisisSomewhat common: Non-violent arguments were somewhat common in narratives describing other relationship crises. The specific causes of these arguments were rarely detailed in the narratives.
Somewhat rare: Friends were most frequently mentioned in other relationship crises, followed by roommates and prospective romantic partners. In some cases, these crises involved violent arguments or instances where the other person filed criminal charges or called the police against the decedent. Additionally, some narratives noted that the crisis stemmed from the decedent being romantically rejected by someone they were interested in.
Rare: In rare cases, the other person in the crisis was described as a step-child, co-worker, intimate partner’s intimate partner, another inmate, neighbor, or a family member’s intimate partner. Rare instances also included situations where the decedent was receiving threats from the other person or facing eviction due to the crisis. A few narratives mentioned that the decedent had general problems with the other person without identifying a specific triggering event.
Other CrisesOther crises are summarized in detail in Supplementary Material Table S5. The four crises in this domain include “School Crisis”, “Disaster Exposure Crisis”, “Physical Health Crisis”, and “Other Crisis”.
Physical Health CrisisSomewhat common: Chronic pain and cancer were the most frequently reported physical health conditions. In several cases, narratives described the decedent experiencing a sudden change in health status, such as receiving a new diagnosis, suffering a medical event (e.g., stroke), or sustaining an injury. It was also somewhat common for the decedent to be in pain at the time of their death.
Somewhat rare: Injuries were less commonly reported. Some narratives also described that the suicide death occurred following a change in the status of a known health condition, such as the worsening of a neurodegenerative disease. Narratives also noted that the decedent had multiple health conditions or had been recently hospitalized before their death.
Rare: In rare cases, the physical health condition associated with the death was noted as a cardiovascular event, neurodegenerative disease, STI, or an unspecified condition. Some narratives described the suicide occurring after a lapse or change in medication, a failed treatment or surgery, or an illness unverified by the decedent’s medical records. Additionally, a few narratives mentioned factors such as addiction to pain medication, medical debt, or the loss of employment, mobility, or independent living due to the illness.
This novel exploratory study examined the contextual details within each of 17 precipitating circumstances preceding adult suicide death, uncovering underexplored risk factors that could serve as targets for intervention efforts. We summarized and reported four main findings including the diversity of circumstances within each category, the ubiquity of interpersonal relationship problems, the influence of crime perpetration, and the potential for misclassification in the crisis variables. Taken together, these results highlight the complexity of suicide death as well as the interconnected nature of circumstantial crises.
Our findings indicate that each category of precipitating circumstance represents a broad and diverse range of experiences. This diversity carries significant implications for screening and prevention efforts and highlights the importance of tailoring interventions that address the underlying causes of each crisis for an individual rather than relying on generalized solutions. This can be illustrated, for example, in the category of eviction crises: 2685 individuals experienced an eviction crisis prior to their death, which might lead researchers to focus on financial and housing support interventions to reduce suicide. However, a closer examination of the narrative circumstances reveals that a notable proportion of these cases were not traditional evictions but instead involved the decedent being “kicked out” of their home due to interpersonal conflicts, substance use, or criminal behavior. For these individuals, housing support alone may be insufficient; instead, interventions such as relationship support or substance use treatment might be more appropriate. As the field of suicide prevention increasingly moves toward complex, multi-level approaches, it becomes critical to balance evidence-based and standardized intervention approaches with the specific and varied needs of individuals.
At the same time, our results highlight that the seventeen crisis variables identified by NVDRS interact and intersect with one another. In 10 of the 17 circumstances, the most common or second most common type of crisis involved an interpersonal relationship. For example, many alcohol-related crises were determined to be arguments with partners, family members, or friends over alcohol use, highlighting that “interpersonal crisis” and “alcohol crisis” may not represent distinct situations, but interconnected experiences. The interconnected nature of such events is supportive of a growing body of literature encouraging researchers to consider suicide from a network, or systems-theory perspective, rather than from a lens of traditional linear cause and effect [13–15]. Future research should further explore a network of precipitating crises to better understand how these factors interact to influence suicide risk. This includes examining the pathways and feedback loops within these networks, as well as identifying potential intervention points that could disrupt escalating cycles of stress. Additionally, whilst the current analysis focused on the acute period preceding the death, events should also be examined in the broader temporal context, considering the additive influence of chronic stressors to garner a full picture of how suicidality builds across the life course.
Perpetration of criminal behavior, including domestic violence, child sex crimes, and DUIs, was prominently represented within 10 of the 17 categories of precipitating circumstances. While much of the existing literature on violent crime and suicide has focused on victims [16], far fewer studies have explored perpetration of crime as a precursor to suicide [17]. One study from the North Carolina VDRS found that 72.7% of domestic violence-related suicide deaths involved the perpetrator [18]. Our findings align with this, showing that in nearly all cases, the person who died by suicide was the perpetrator of the violence. There are several theories that seek to explain this correlation, including suicidal behavior as a maladaptive coping strategy for interpersonal stress [19,20], neurobiological links between aggression and suicidality [21,22], or aggression as an independent manifestation of the shared risk factors with suicidality [18]. Another particularly striking result of our study was the significant influence of child sex crimes, including viewing child sexual abuse material and committing abuse themselves. Among individuals experiencing a criminal crisis at the time of their death, 20% of cases in this study were linked to the perpetration of child sex crimes. Moreover, these behaviors emerged as salient themes across other crisis categories, including “other addiction” crises, eviction crises, civil legal crises, and “other relationship” crises. While it is known that individuals who engage in these behaviors may be at higher risk of suicide than the general population [23–25], our findings suggest that the proportion of deaths linked to these acts may be higher than previously reported. Overall, the ubiquity of crime perpetration across these results suggests a need for further research into crime-related suicide, particularly to identify which offenders are at heightened risk and pinpoint the stages within the criminal justice process where risk is greatest, enabling more targeted assessment and intervention efforts.
Lastly, this analysis highlighted the potential for misclassification and coding discrepancy among the crisis variables, particularly regarding the timing of events. Though the NVDRS indicates that the crisis variables should be coded as present if the circumstance occurred within the two weeks surrounding the death, the use of this threshold varied according to the circumstance. For example, if the decedent’s parent had died by suicide three months ago, but the decedent was still actively grieving at the time of their death, this was typically still considered a crisis. Additionally, some circumstance categories (particularly “other” crisis, alcohol use crisis and substance use crisis) had large numbers of narratives with no indication that a crisis had occurred at all preceding the death. These issues were particularly evident among those who experienced “other crises”, with 61% of narratives in this category misclassified. This study was not intended as a formal validation of the crisis variables, but these findings highlight the need for such a study to maximize the validity of NVDRS data.
Implications for Suicide PreventionThis study’s findings underscore the need to rethink current suicide prevention efforts, which predominantly focus on mitigating psychological conditions, such as depression [26,27]. While addressing mental health is an important aspect of suicide prevention, such an approach is insufficient on its own, given that a substantial proportion of suicide deaths occur among individuals with no known psychological illness [28].
The results of this study suggest several novel areas where interventions could be targeted that would benefit all decedents, such treatment for alcohol use disorder, support for non-violent familial arguments, or postvention support for bereavement, all of which were identified as “very common” circumstances in the analyzed narratives. Interventions of this nature are currently lacking. For example, one systematic review by Andriessen, et al. sought to assess the evidence of the effectiveness of interventions for people bereaved by suicide death, finding that only two studies considered suicidal ideation as an outcome, and that only one demonstrated any significant effect [29]. A similar dearth of evidence was found in a review by Kolva et al., which identified that whilst there were empirically supported interventions that target psychological distress in patients with cancer, only four had been tested in the context of suicidal ideation [30]. These gaps present an opportunity for the development of targeted intervention strategies across a variety of precipitating circumstances to address these underexplored risk factors.
Strengths and LimitationsOur study is subject to limitations which should be considered in the interpretation of the results. First, the NVDRS narrative data is derived from coroner/medical examiner and law enforcement reports, which have been shown to vary in quality and depth, reflecting the fragmented nature of the US death investigation system, differences in investigative practices, and reporting [31]. This variability means that some precipitating circumstances or their causes may be under- or over-represented in these results based on the likelihood of their being reported in the source material, or by demographic characteristics [32].
Additionally, while more comprehensive than other available data sources, the NVDRS narratives still lack granularity and detail. For example, of the 48 intimate partner crises that were related to an argument, less than half of narratives mentioned the cause of the argument. In the rest of the cases, we know an argument occurred but we do not know what it was about, limiting our understanding of specific stressors within these relational dynamics. Even the most robust narratives are unlikely to have captured the depth and scope of any individuals’ stressors.
Finally, while these results identify contextual factors embedded in precipitating circumstances, we cannot attribute these factors as causal in any death. The documented events in these narratives were known to have occurred, but they were reported by third parties (e.g., next-of-kin, law enforcement). Thus, we cannot fully ascertain whether any specific event or combination of events was truly a driving circumstance in a suicide death. Additionally, this study represents an initial exploration of these data and methods, and while it provides valuable insights into crisis circumstances preceding suicide, it did not examine how these events may differ by important characteristics known to influence suicide deaths such as sex, age, race/ethnicity, mental health status, or lethal means. Future research should investigate how the narrative context may differ in such groups.
Despite the limitations of the dataset, this work highlights a variety of underexplored circumstances and recognizing the complexity that is salient in suicide death. These results ultimately invite researchers to carefully consider how circumstance variables are operationalized when they are used in future studies, leading to more nuanced interpretations of these variables and, ultimately, to more targeted prevention strategies.
To protect the identities of the decedents, no specific quotations or stories are shared and all identifying details are censored. Rather, generalized examples are reported. This project was approved by the CDC-NVDRS, and was determined not to be human subjects research by the Institutional Review Board at the University of Iowa (Project ID: 202504806).
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Table S1: Addiction-related crises, Table S2: Economic Crises, Table S3: Court-related Crises, Table S4: Relationship-related Crises, Table S5: Other Crises.
The NVDRS is publicly available to researchers and public health practitioners at https://www.cdc.gov/nvdrs/about/nvdrs-data-access.html.
Conceptualization, AS, ER, SN, AS, JT, JP; Methodology, AS, SN, JP; Software, AS; Validation, AS, ER, SN, AS, JT, JP; Formal Analysis, AS; Investigation, AS, JP; Data Curation, AS, JP; Writing—Original Draft Preparation, AS, SN, JP; Writing—Review & Editing, AS, ER, SN, AS, JT, JP; Visualization, AS, SN, JP; Supervision, JP.
The authors declare that they have no conflicts of interest.
The authors report this research received no external funding.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
Sursely A, Nash S, Sadler A, Roberts E, Torner J, Platt J. Exploring contextual details in suicide precipitating circumstances: A qualitative content analysis of national violent death reporting system (NVDRS) narrative reports. J Psychiatry Brain Sci. 2025;10(4):e250008. https://doi.org/10.20900/jpbs.20250008.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




