Location: Home >> Detail
J Psychiatry Brain Sci. 2025;10(5):e250012. https://doi.org/10.20900/jpbs.20250012
 ,
David Ramírez-Saco 2,3 ,
Ruth Cunill 4 ,
Magí Farré 1,5 ,
Marc Saez 6,7,8 ,
Xavier Castells 3
,
David Ramírez-Saco 2,3 ,
Ruth Cunill 4 ,
Magí Farré 1,5 ,
Marc Saez 6,7,8 ,
Xavier Castells 3
1 Department of Pharmacology Therapeutics and Toxicology, Universitat Autònoma de Barcelona, Bellaterra 08193, Spain
2 Department of Clinical Pharmacology, Vall d’Hebron Barcelona Hospital Campus, Barcelona 08035, Spain
3 TransLab Research Group, Department of Medical Sciences, University of Girona, Girona 17004, Spain
4 Sant Joan de Deu-Numancia Health Park, Barcelona 08029, Spain
5 Department of Clinical Pharmacology, Hospital Universitari Germans Trias i Pujol, Badalona 08916, Spain
6 Center for Research in Health and Economics (CRES), Economy and Business Department, Universitat Pompeu Fabra, Barcelona 08005, Spain
7 Research Group on Statistics, Econometrics and Health, University of Girona, Girona 17004, Spain
8 CIBER of Epidemiology and Public Health (CIBERESP), Madrid 28029, Spain
* Correspondence: Maggie Barcheni
Placebo and nocebo effects are psychological and physiological phenomena that significantly impact clinical trial outcomes, particularly in psychiatric disorders. While extensively studied individually, their interplay remains unexplored. This study investigates the relationship between placebo and nocebo responses in Attention Deficit Hyperactivity Disorder (ADHD) to improve the design and validity of Randomized Placebo-Controlled Clinical Trials (RPCCTs). This study is a secondary analysis of two previously published systematic reviews investigating placebo and nocebo responses in ADHD. A meta-regression analysis was conducted using data from 71 RPCCTs involving 6205 participants. Placebo response was measured as changes in ADHD symptom severity, while nocebo response was defined by the incidence of adverse events (AEs) in placebo groups. Multivariate analyses were used to explore the correlation between placebo and nocebo responses, adjusting for trial-level covariates. Placebo responses were positively associated with comorbidity as an inclusion criterion, psychotherapy, intention-to-treat analysis, and high risk of bias, and negatively associated with the number of study centers, use of a parallel design, and trials conducted in the U.S.
Nocebo responses were positively associated with treatment naivety, treatment duration, proactive adverse event collection, and high risk of bias. The multivariate analysis showed no significant correlation between placebo and nocebo responses (coefficient = 0.0034, p-value = 0.8881) in ADHD trials. These findings challenge assumptions regarding the interdependence of placebo and nocebo responses and highlight the need for independent consideration of these phenomena in clinical trial design. Understanding these mechanisms can contribute to refining trial methodologies and optimizing therapeutic outcomes for ADHD. Further research is needed to explore whether this lack of correlation extends to other psychiatric disorders.
Placebo and nocebo effects are well-established psychological and physiological phenomena mediated by mechanisms such as conditioning and expectancy. Conditioning involves prior experiences with an active substance, creating a memory trace that enables an inert substance to elicit a similar physiological effect. Expectancy reflects how a patient’s beliefs influence their perceived treatment outcomes, aligning observed changes with their expectations even when receiving an inactive intervention [1,2]. While placebo effects improve symptoms, nocebo effects worsen them [3,4]. In this study, we define placebo response as the total symptom improvement observed in the placebo arms of randomized controlled trials. This response includes a combination of contributors, such as expectancy mechanisms, regression to the mean, spontaneous remission, and non-specific contextual factors [5,6]. In contrast, the placebo effect refers more narrowly to psychobiological mechanisms, such as expectancy and classical conditioning, that contribute to improvement in the absence of active pharmacological treatment [1,3]. This distinction is critical in interpreting placebo-related outcomes in clinical research.
Psychological factors leading to direct placebo and nocebo effects are important contributors to placebo and nocebo responses; however, their causes and explanations also extend to natural disease progression, variability in measurement, and mathematical phenomena like regression toward the mean.
Clarifying distinctions between placebo and nocebo effects and responses is essential for understanding their clinical implications. These responses, though well-documented in conditions like major depression [7,8], are under-researched in other psychiatric disorders, such as bipolar disorder [9], schizophrenia [10], and ADHD [11]. This knowledge gap is significant because high placebo and nocebo responses can obscure the true efficacy of treatments in RPCCTs, undermining their validity.
While some authors have expressed concern that high placebo responses contribute to trial failure and hinder drug evaluation, others have shown that placebo and drug responses often rise in parallel, preserving effect sizes [12–14]. This challenge exacerbates the broader “crisis” in psychopharmacology by complicating treatment evaluation and hindering the clinical development of new medications for brain disorders, leading to a decline in research and innovation [15,16]. We acknowledge these differing perspectives and have aimed to present a balanced interpretation of placebo response trends in clinical trials.
Placebo and nocebo responses have become critical areas of medical research, particularly in psychiatry, where patients’ beliefs about treatment can profoundly shape clinical outcomes. In conditions like depression and anxiety disorders, placebo responses can amplify perceived treatment efficacy, while negative expectations in chronic pain and anxiety disorders can heighten AEs through the nocebo effect [17,18]. Similarly, placebo and nocebo responses modulate symptom severity in disorders such as irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD) [19,20] and have even been linked to immune and allergic responses [21,22].
ADHD is a neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsivity [23]. It carries substantial clinical and social consequences, including an increased risk of substance use disorder [24], accidents [25], and premature mortality [26]. Despite the well-documented influence of placebo and nocebo responses in psychiatric disorders, their role in ADHD remains underexplored. Recent research suggests that ADHD clinical trials may be particularly susceptible to these responses [27], but whether they interact or occur independently has yet to be determined.
While placebo and nocebo effects have been extensively studied individually, no research has systematically examined the relationship between placebo and nocebo responses in ADHD. Recent meta-analytic evidence, however, has shown that ADHD demonstrates strong placebo responses but weak nocebo responses, particularly when measured by dropout rates due to AEs [28]. This discrepancy further highlights the need to better understand whether these responses are related or independent in psychiatric trials. Understanding this interplay is crucial because both responses significantly impact clinical trial outcomes by influencing symptom perception, treatment adherence, and overall trial validity. High placebo responses can obscure the true efficacy of pharmacological treatments, while high nocebo responses may undermine their safety, complicating risk-benefit analyses. Investigating their relationship will provide valuable insights into whether these responses share underlying mechanisms or occur independently. Given the absence of prior studies on this topic, our research represents the first empirical exploration of this relationship, offering a novel contribution to the field and informing future clinical trial design.
This study aims to bridge this gap by investigating the relationship between placebo and nocebo responses in ADHD. We hypothesize that placebo and nocebo responses show a positive correlation, meaning that trials with stronger placebo responses also exhibit stronger nocebo responses. By analyzing this relationship, we aim to contribute to the design of more robust RPCCTs and enhance therapeutic strategies for individuals with ADHD.
This is a secondary analysis of two previously published systematic reviews with meta-analyses investigating placebo [27] and nocebo [29] responses in ADHD and the effect of their predictors. Both systematic reviews included RPCCTs investigating the efficacy and safety of any pharmacological intervention investigated for ADHD patients, diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) III–R, DSM–IV, IV–TR or 5, irrespective of age. To be included, RPCCTs had to provide data on the efficacy on ADHD symptoms using an 18-item, clinician-rated, DSM-based ADHD rating scale scoring from 0 to 54 points; additionally, the incidence of any AE had to be reported and the double-blind phase had to last at least 1 week.
Withdrawal RPCCTs, studies detailed as congress abstracts were excluded as well as RPCCTs with a drug lead-in phase and those investigating interventions targeting symptoms other than the ADHD core ones, e.g., studies investigating antipsychotics for aggressiveness in ADHD patients.
Source of DataData were extracted from Minerva Database [30] on 01/11/2023. Minerva Database (Minerva Database, 2021) stores comprehensive information on all RPCCTs that have investigated the efficacy and safety of pharmacological interventions for ADHD, updating each week from Medline, CENTRAL, and PsycINFO.
Study VariablesThe primary outcomes were the nocebo response (dependent variable) and the placebo response (independent variable). The nocebo response was defined as the proportion of patients reporting AEs while receiving a placebo. The placebo response was measured as the change from baseline in ADHD symptom severity, using an 18-item clinician-rated ADHD rating scale aligned with DSM-IV, IV-TR, or DSM-5 criteria. This scale employs a 4-point severity rating for each item, with higher scores indicating greater symptom severity. Notably, placebo response values often appear as negative, signifying symptom improvement from baseline. These definitions distinguish the observed responses from placebo and nocebo effects, which involve the mechanisms underlying these changes, such as conditioning and expectancy.
Covariates: We collected the following covariates: patient age (mean age within each RPCCT), gender distribution (proportion of male patients in each RPCCT), ethnic composition (proportion of Caucasian patients in each RPCCT), baseline ADHD severity (mean baseline score on the DSM-based ADHD-RS), treatment naivety (categorized as “yes” or “no”), type of drug (psychostimulant or non-stimulant), treatment regimen (fixed or flexible dose), treatment duration (in weeks), Intention to Treat analysis (categorized as “yes” or “no”), concomitant psychotherapy (administered or not), legal status of the drug (approved or non-approved), number of study sites, probability of receiving a placebo (expressed as a ratio of patients who received placebo to the total number of patients in each RPCCT, in percentage), study design (parallel or crossover), comorbidity as an inclusion criterion (categorized as “yes” or “no”), method for collecting AEs (open or systematic), publication year, geographical region (USA included or excluded), and an assessment of the risk of bias (see next section).
Risk of Bias AssessmentTo assess the risk of bias within each included study, the Cochrane Risk of Bias Tool was employed. This tool evaluates the risk of bias across seven domains, including sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias. The risk of bias in each domain is categorized as “low,” “high,” or “unclear”.
Statistical AnalysisFirst, missing data were imputed using Multiple Imputation by Chained Equations (MICE) [31]. Then, we conducted a detailed descriptive analysis of the included RPCCTs, examining various patient, intervention, and study characteristics. We utilized the method of moments–based meta-regression to ascertain the relationship between each study covariate and both the placebo and nocebo responses separately. Afterwards, we explored the association between placebo and nocebo responses through multivariate meta-regression. The selection of covariates for inclusion in this analysis was based on previous univariate analyses, so that those covariates associated at least at a statistical trend (p-value below 0.1) with both placebo and nocebo responses were included in the multivariate meta-regression model in which significance was set at p-value <0.05. The statistical software Comprehensive Meta-Analysis v3 was used for all meta-regression analyses.
This study involved a comprehensive examination of 71 RPCCTs encompassing a total of 6205 participants who received placebo. No covariates were excluded due to insufficient information, and missing data were addressed through imputation, reflecting a distribution akin to observed data. Covariates were found to be non-collinear, ensuring their relevance in the analysis. The patient demographic profile (see Table 1) revealed a mean age of 21.3 years, with a predominantly male (64.2%) and Caucasian (72.4%) population. ADHD symptom severity at baseline ranged from moderate to severe. Non-stimulant drugs were predominantly investigated, and over half of the studies adopted a flexible dosing regimen. The average treatment duration was 7.0 weeks. Psychotherapy was infrequently provided concurrently, and most interventions investigated were approved for ADHD treatment. Study characteristics highlighted a multicenter approach, and a prevalent parallel design. Pharmacological naivety and comorbidity as inclusion criteria were uncommon. The probability of receiving placebo averaged 36.1%, and systematic methods were widely utilized for adverse event collection. The dataset predominantly featured studies published in 2006 or later, with a significant proportion conducted in the USA. A limited number of RPCCTs were considered to have a high risk of bias, with attrition bias due to high dropout rates among placebo-receiving patients being the most prevalent source of bias. Across the 71 included trials, the average proportion of participants in the placebo group who reported at least one adverse event was 55.5%, with a wide range from 4.2% to 90.2% (I² = 88.3%), indicating substantial heterogeneity.
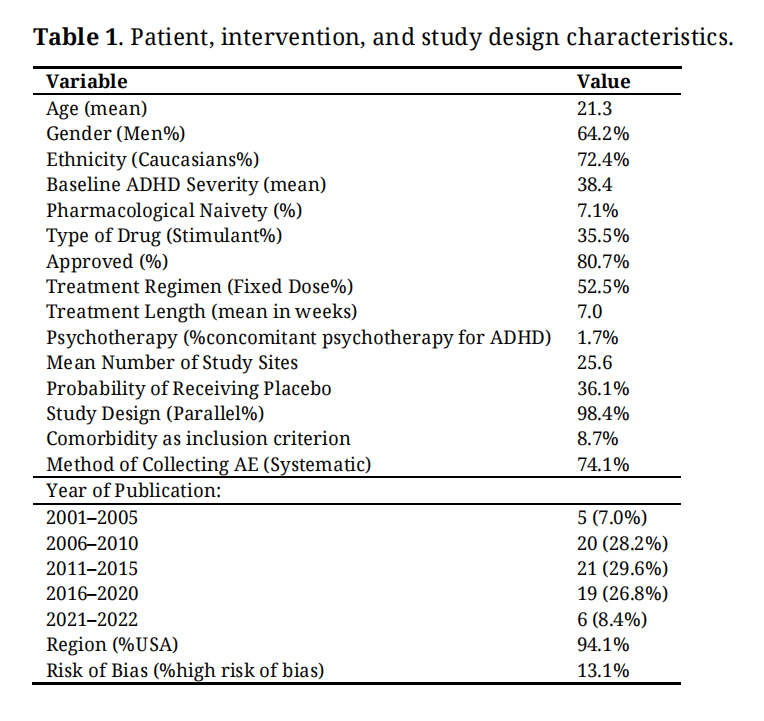 Table 1. Patient, intervention, and study design characteristics.
Table 1. Patient, intervention, and study design characteristics.
We conducted a comprehensive bivariate analysis to assess the impact of various factors on the placebo and nocebo responses. Table 2 presents the coefficients, standard errors, and p-values associated with each covariate. Notably, several factors demonstrated statistical significance (p < 0.05). For the placebo response, comorbidity as an inclusion criterion exhibited a significant positive effect (Coefficient = 3.4269, p-value = 0.0031), suggesting a substantial association. High risk of bias (Coefficient = 2.1261, p-value = 0.0274) and Intention-to-Treat (ITT) analysis (Coefficient = 2.3841, p-value = 0.0071) also emerged as significant contributors. Conversely, the number of centers negatively influenced the placebo response (Coefficient = −0.0756, p-value = 0.0001), indicating a noteworthy association. Moreover, Psychotherapy (Coefficient = 7.83, p-value = 0.0292) and Region (Coefficient = −2.9547, p-value = 0.0036) demonstrated significant impacts. Regarding the nocebo response, several factors emerged as statistically significant contributors. High Risk of Bias (Coefficient = 0.3845, p-value = 0.0357), treatment length (Coefficient = 0.0592, p-value = 0.000) and naive as an inclusion criterion (Coefficient = 0.6183, p-value = 0.0076) all showed significant positive impacts. Additionally, Proactive AE collection (Coefficient = 0.6794, p-value = 0.0000) exhibited a significant positive association, whereas publication date (measured in days) showed a statistically significant but negative association (Coefficient = −0.0001, p-value = 0.0001).
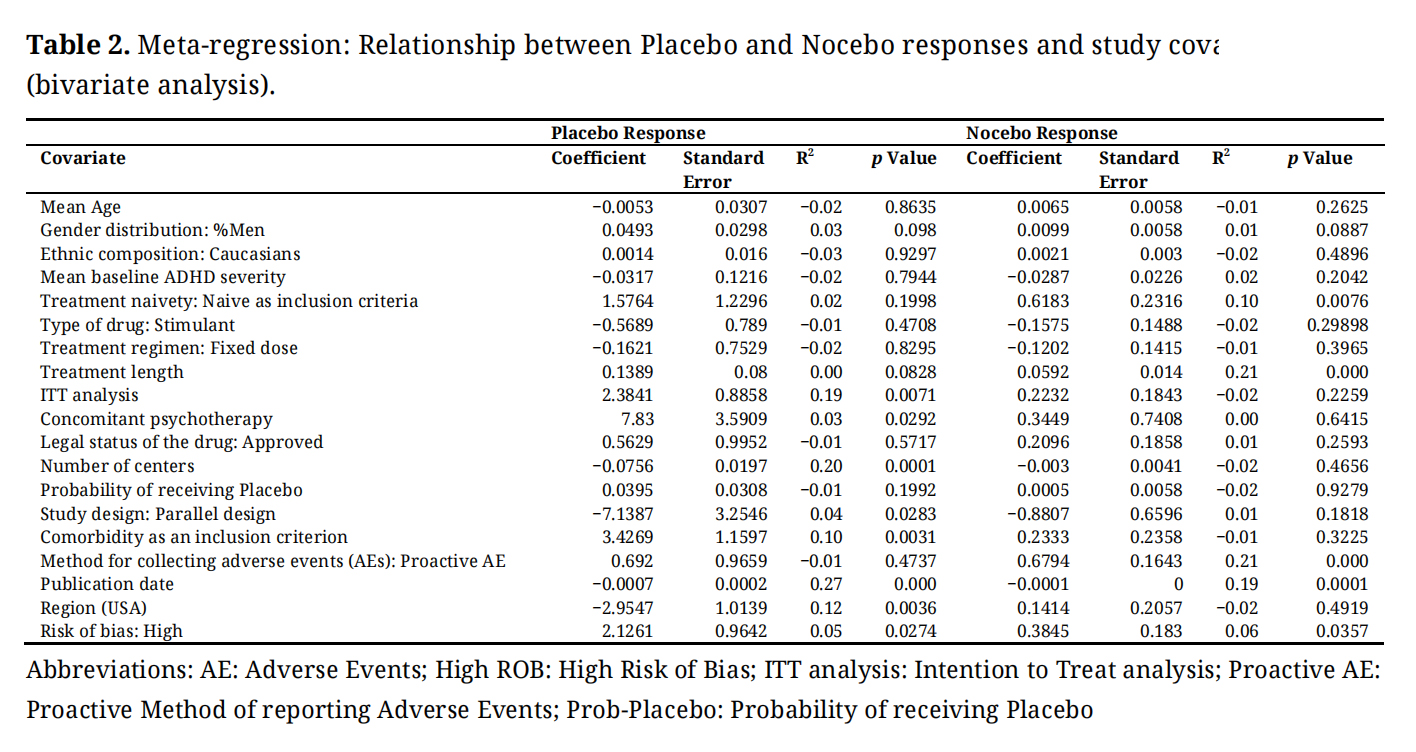 Table 2. Meta-regression: Relationship between Placebo and Nocebo responses and study covariates (bivariate analysis).
Table 2. Meta-regression: Relationship between Placebo and Nocebo responses and study covariates (bivariate analysis).
The association between placebo and nocebo responses was analyzed through multivariate meta-regression in which covariates found to be associated with both the placebo and nocebo responses; high risk of bias and publication date, were included in the analysis. Upon conducting the multivariate analysis (Supplementary Table S1), a key finding emerged: no statistically significant association was found between the placebo and nocebo responses (coefficient = 0.0034, p-value = 0.8881). This lack of association is also visually represented in Figure 1, which shows the relationship between placebo and nocebo responses across the included trials.
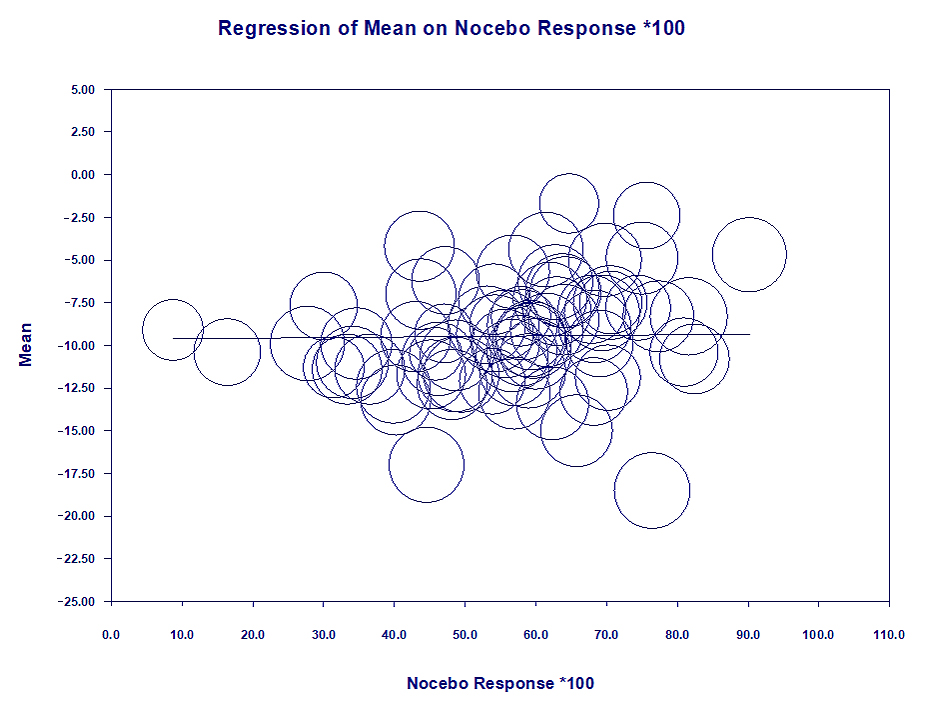 Figure 1. Co-relationship between Placebo and Nocebo response.
Figure 1. Co-relationship between Placebo and Nocebo response.
This study provides the first analysis of the relationship between placebo and nocebo responses in ADHD, collecting data from 71 RPCCTs involving 6205 participants. Contrary to our hypothesis, multivariate meta-regression revealed no statistically significant correlation between these responses, even after adjusting for potential confounders. Our hypothesis had been based on theoretical models suggesting that shared psychological mechanisms—particularly expectancy and conditioning—could drive both symptom improvement and adverse event reporting. From this perspective, higher suggestibility or stronger treatment expectations could amplify both placebo and nocebo responses simultaneously, leading to a positive correlation. However, we acknowledge that alternative hypotheses are also plausible—for instance, that negative expectancy might inhibit placebo-related improvement, resulting in a negative association. Our null finding, therefore, challenges both assumptions and highlights the complexity of these phenomena. It also suggests that placebo and nocebo responses may be governed by partially independent processes, at least in the context of ADHD clinical trials.
This lack of correlation is further supported by the distinct set of covariates influencing each response. In our bivariate analyses, placebo response was positively associated with intention-to-treat analysis, psychotherapy, comorbidity as an inclusion criterion, and high risk of bias. It was negatively associated with the number of study centers, use of a parallel design, and trials conducted in the U.S. In contrast, nocebo response was positively associated with treatment naivety, treatment duration, proactive AE collection, and high risk of bias. These distinct patterns suggest that placebo and nocebo responses are influenced by different mechanisms and trial-level features. These differences suggest that placebo and nocebo responses operate through separate mechanisms, as reflected in their distinct predictors.
The nature of our data does not allow for a definitive explanation of this lack of correlation. However, our findings challenge the assumption that placebo and nocebo responses are interdependent—at least in ADHD—and suggest that these responses are driven by different processes rather than a shared underlying effect. One possible explanation is that ADHD symptoms naturally fluctuate over time [6], making symptom changes in RPCCTs largely attributable to this variability rather than a true placebo effect. This could diminish the overall impact of placebo mechanisms on symptom reduction, contributing to the observed lack of correlation between placebo and nocebo responses. However, as our study focuses specifically on ADHD, further research is needed to determine whether these findings extend to other conditions, particularly those with more stable symptom progression.
Our findings have important implications for RPCCT design in ADHD research. Given the independent nature of placebo and nocebo responses, these phenomena should be treated as separate entities in clinical trial design. Strategies to reduce placebo responses (e.g., minimizing expectancy biases, stricter inclusion criteria) should not be assumed to affect nocebo responses. Likewise, interventions to reduce nocebo responses (e.g., improved adverse event framing, participant education) should not be presumed to alter placebo effects. Furthermore, statistical models should analyze placebo and nocebo responses independently to ensure their unique contributions to trial outcomes are accurately assessed. Finally, the natural variability of ADHD symptoms necessitates careful trial planning, including extended baseline observation periods, longer trial durations, and stratified analyses based on baseline severity and comorbidities, to improve the reliability of results.
While our study provides valuable insights into placebo and nocebo responses in RPCCTs of ADHD treatments, several limitations should be considered. One notable limitation of our study is the potential for ecological fallacy. Despite the comprehensive examination of 71 RPCCTs involving 6205 participants who received placebo, it is essential to acknowledge that our findings are derived from aggregated trial-level data. The ecological fallacy arises from the assumption that individual-level associations between variables hold true at the aggregate level, which may not always be the case [32]. This bias can affect the generalizability of our results to individual patients within each trial. Future research should aim to overcome this limitation by employing study designs that collect individual-level data and analyze relationships or outcomes accordingly. Furthermore, certain categories, such as region or comorbidities, exhibit skewed distributions. To address class imbalance, we aggregated studies into broader categories such as “not US” or “comorbidity as an inclusion criterion” for the meta-regression. While this approach facilitates statistical analysis, it comes at the cost of reducing the granularity of the information analyzed. Additionally, while we conducted statistical analyses to assess the impact of various factors on placebo and nocebo responses, the choice of covariates and statistical methods may have limitations; some important covariates may have been omitted, for example, illness duration [33], which is usually not reported in ADHD trials. To address potential limitations in our study, robust imputation methods were employed for handling missing data, ensuring a distribution akin to observed data. Recognizing the potential constraint on external validity due to the predominant inclusion of studies from the USA, efforts were made to extrapolate findings cautiously. Finally, to gain a deeper understanding of the placebo response, it would be helpful to compare the changes in ADHD symptoms between patients receiving placebo and those receiving no intervention. However, none of the studies included in our meta-analysis utilized such a design.
This study is the first to systematically explore the relationship between placebo and nocebo responses in ADHD clinical trials. By revealing the independence of these responses, we challenge the assumption about their interplay and provide a novel framework for understanding their distinct roles in clinical research. Our findings emphasize the importance of addressing placebo and nocebo responses separately in future trial designs. Future research with individual-level analyses is required to confirm our findings.
Ethical review and approval were waived for this study, as it is a meta-analysis of aggregated data retrieved from the Minerva database. In addition, the work represents a secondary analysis of a previous study conducted by our research group.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Table S1: Meta-regression: Relationship between Nocebo Response and study covariates (multivariate analysis).
The dataset generated from (or analyzed in) the study can be found at Minerva Database. Available from: https://minervadatabase.org/en.
Conceptualization: MB, XC; Methodology: MB; Validation: MB, XC, DR; Formal Analysis and Data Curation: MS; Writing—Original Draft Preparation: MB; Writing—Review & Editing: MB, XC, DR, RC, MF, MS; Supervision: XC.
Not Applicable.
Not Applicable.
The authors declare no conflicts of interest related to this work. The first author began their current employment after the completion of the research, data analysis, and manuscript preparation. During the conduct of this study, the author participated as an independent researcher. The employer had no role in any aspect of the study.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Barcheni M, Ramírez-Saco D, Cunill R, Farré M, Saez M, Castells X. A secondary meta-regression analysis of the relationship between placebo and nocebo responses in ADHD trials. J Psychiatry Brain Sci. 2025;10(5):e250012. https://doi.org/10.20900/jpbs.20250012.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




