Location: Home >> Detail
J Psychiatry Brain Sci. 2025;10(4):e250011. https://doi.org/10.20900/jpbs.20250011
 ,
Huei-Yang Chen 1
,
Huei-Yang Chen 1
1 Neurodegenerative Disorders Research Pty Ltd., West Perth, WA 6005, Australia
2 School of Medicine, The University of Western Australia, Nedlands, Crawley, WA 6009, Australia
* Correspondence: Peter K Panegyres
Background: Young onset dementia, with onset prior to 65 years, is an enigmatic condition when it occurs in the absence of gene mutations and recognized risk factors. The aim of this study is to determine if self-reported psychosocial stressors might be implicated.
Methods: For over 25 years we have been prospectively evaluating the neurobiology of YOD. Patients are diagnosed using published criteria. The presence of self-reported psychosocial stressors was investigated by direct enquiry from patient, spouse and family, and had to be stable at six months to be recorded as psychosocial stressors. This study incorporates 221 participants. Patients and their families were asked standardized questions developed by the senior author. The same questions were asked by the cognitive raters. A stress was rated as a stressor if confirmed by both neurologist and cognitive rater and at follow-up visit.
Results: Of the 131 individuals with sporadic young onset Alzheimer’s disease, 59.5% had psychosocial stressors compared to 3% of old onset AD (p < 0.001), and 50% of the 46 individuals with sporadic behavioral variant frontotemporal dementia had psychosocial stressors in comparison to 3.3% of old onset (p < 0.00001). Only 2% of age-matched controls without dementia reported psychosocial stressors.
Conclusions: Our findings suggest that psychosocial stressors may be a risk factor for YOD and point to early intervention. The results also suggest that the physico-chemical properties of the physiological reactions to psychosocial stress activate neurodegenerative pathways.
AD, Alzheimer’s disease; bvFTD, behavioral variant frontotemporal dementia; CAA, cerebral amyloid angiopathy; LBD, Lewy body disease; PCA, posterior cortical atrophy; PNFA, progressive non-fluent aphasia; PPA, primary progressive aphasia; PSP, progressive supranuclear palsy; PTSD, Post-traumatic stress disorder; SD, semantic dementia; YOAD, young onset Alzheimer’s disease; YOD, young onset dementia.
We have a long-standing interest in the neurobiology of YOD [1]. We have been intrigued by the mechanisms that might determine its development. Our earlier studies on a smaller cohort suggested that hypertension and a single apolipoprotein ε4 allele might be important risk factors. Investigations of larger cohorts by our group disclosed that elevated inflammatory markers, impaired renal function and APOE ε4 alleles were over-represented in those whose onset of AD was greater than 65 years [2]. Ethnic factors seem to be relevant with African Americans more likely to develop young onset AD (YOAD). Our earlier studies also suggested that YOAD is independent of the development of hypertension, stroke and atrial fibrillation [3]. Our genetic studies showed that most subjects did not have a family history and YOAD was not strongly inherited as an autosomal dominant trait; gene mutations were an uncommon cause, found in less than 10% [4]. These findings led us to the conclusion that YOAD is driven by stochastic forces and permeate at a DNA, RNA or protein level [1,5].
Theoretically, increased levels of stress switch on the hypothalamic-pituitary-adrenal axis (HPA) which increases cortisol. This elevated cortisol aggravates AD and the AD pathophysiology disrupts stress control circuits, resulting in more stress and additional neurodegeneration; advancing neurodegeneration causing anxiety, depression, insomnia and malaise. Stress also increases Aβ and neuritic plaque deposition, as well as the deposition of phosphorylated tau [6]. Neuroinflammation is augmented by stress which further aggravates neurodegeneration, along with stimulation of the sympathetic nervous system [7]. Aberrations of the HPA with elevated cortisol and amplification of neuroinflammation enable the hippocampus and other neuronal systems vulnerable to neurodegeneration and the deposition of Aβ and tau. Stress might also act on microglia to promote neurodegeneration [8]. These stress systems encouraged us to search the relationship between stress and YOD.
Psychosocial stressors represent an interplay between the external world and inner emotional reactions resulting in a stress reaction. Psychosocial stressors may be associated with: employment; other people; life circumstances (e.g., divorce, chronic illness, relocation, altered career path); catastrophic events (e.g., assault, war, natural disaster); the daily struggle (e.g., job requirements); or chronic conditions (poverty, racial discrimination, competitive work, environmental pollution, climate change). All of these life events can activate neurodegenerative pathways.
Recent studies of 356,052 individuals in the United Kingdom BioBank revealed that minimal alcohol use, higher formal education and lower physical frailty reduced risk of YOD, but a low socio-economic, APOE-ε4 status, alcohol use disorder, social isolation, vitamin D deficiency, elevated C-reactive protein, deafness, orthostatic hypotension, stroke, diabetes, heart disease and depression did not [9]. Larger N numbers and differences in methodology might explain the differences between our findings and those results. This study and our previous enquiries have not investigated the role of psychosocial stress as a potential modifiable risk factor [1,3,10,11]. This study sets out to correct these deficiencies, which might be missing in large cohort studies, and investigate the null hypothesis that there is no relationship between psychosocial stress and YOD.
It is now some 25 years of the ARTEMIS Project which is an ongoing prospective evaluation of the neurobiology of YOD {JHC HREC: ARTEMIS 1406}. The project is performed in community-based centers established by the senior author who is affiliated with the University of Western Australia. Perth is Australia’s fourth largest city and is the capital of Western Australia, and is one of the world’s most isolated cities. It was founded by the British, which reflects that over 50% of the population are of British and Irish ancestry. All the patients included in this study were of British-Irish origin and resided in Perth. The median weekly income in Australian dollars is indicative of high socio-demographic index [12]—personal AUD$859; family AUD$2259; and households AUD$1.865. These clinics are devoted to the diagnosis, management and long-term follow-up of patients with YOD with onset prior to 65 years. The patients are referred to the centres by general practitioners, psychiatrists, neurologists, geriatricians and other physicians. Patients and their families are seen at least six-monthly, or more frequently depending on clinical need (follow-up median 11 years, range 1–15 years). The patients’ diagnoses were based on published criteria and made by the same neurologist, psychiatrists, neuropsychologists, cognitive raters and case managers, who were also involved in the patients’ long-term care. This study only includes those with sporadic YOD and old onset dementia with onset greater than 65 years, and non-demented controls. All patients and their carers gave written informed consent.
Assessments of Psychosocial StressAt first assessment patients and their families were asked standardized questions developed by the senior author (if English was not the first language, an official interpreter was used, unrelated to the patient):
1.
2.
3.
The same phraseology was used by Investigator and cognitive raters. The cognitive raters were trained by the Principal Investigator to use the same wording as shown. The presence of stressors was confirmed by regular meetings at six-monthly intervals and at subsequent clinical visits. Patients were asked about the developments of new stressors at each follow-up visit. A stress or stressors were confirmed as present if identified by the Investigator and cognitive rater/s; both had to be in complete consensus for a stress or stressors to be categorized. Furthermore, the stress or stressors had to be established at follow-up. Monthly meetings between Investigator and raters settled the findings.
The methods of diagnosis and criteria used in this cohort have previously been published [1].
AnalysesData was examined using the Chi-square test and Fisher’s Exact Test.
There is a statistically significant increase in the frequency of psychosocial stressors in patients with YOAD (Table 1, p < 0.001). Similarly people with bvFTD had increased psychosocial stressors (p < 0.00001). Patients with other forms of dementia, such as linguistic variant FTD, PPA and SD had a trend to increased frequencies but did not achieve statistical significance. Similarly, patients with PSP, LBD and PCA shifted towards an association but did not reach statistical significance. Age-matched controls without dementia were also studied, where there were only 2 subjects who reported psychosocial stressors.
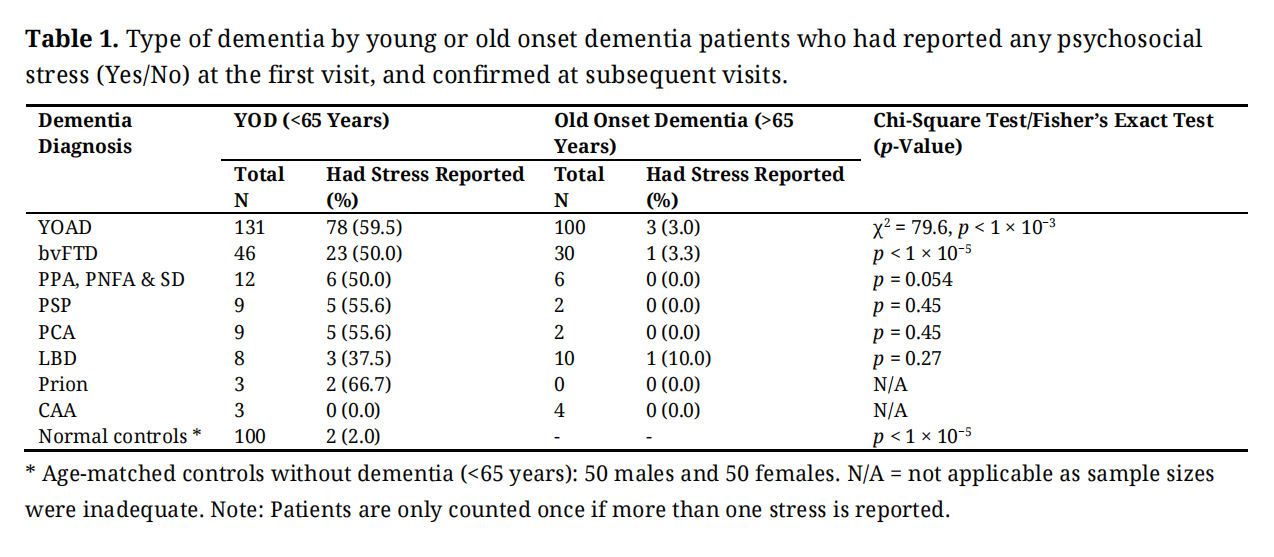 Table 1. Type of dementia by young or old onset dementia patients who had reported any psychosocial stress (Yes/No) at the first visit, and confirmed at subsequent visits.
Table 1. Type of dementia by young or old onset dementia patients who had reported any psychosocial stress (Yes/No) at the first visit, and confirmed at subsequent visits.
The types of psychosocial stressors included, in order of frequency: family or personal illness, loss of a loved one, lack of resources for adequate survival, social isolation, job stress and relationship difficulties (Table 2)—see Supplementary Table S1 for detailed listing of the types of psychosocial stressors. In our patients, lack of resources for adequate survival included: loss of employment, low income and loss of income; and relationship difficulties encompassed infidelity, domestic violence and financial stress.
Some patients had more than one psychosocial stress reported at the time of the first visit. Seventeen patients with YOAD had 2, and eight had 3. This is in contrast to patients with bvFTD and linguistic presentations of FTD: PPA, SD, which had lower numbers of 2 or 3 stressors (Table 3). The other diagnostic categories had only one stress, with five patients in the non-neurodegenerative group having 3 stressors. YOAD patients had the greatest number of people with 2 or more stressors (N = 28).
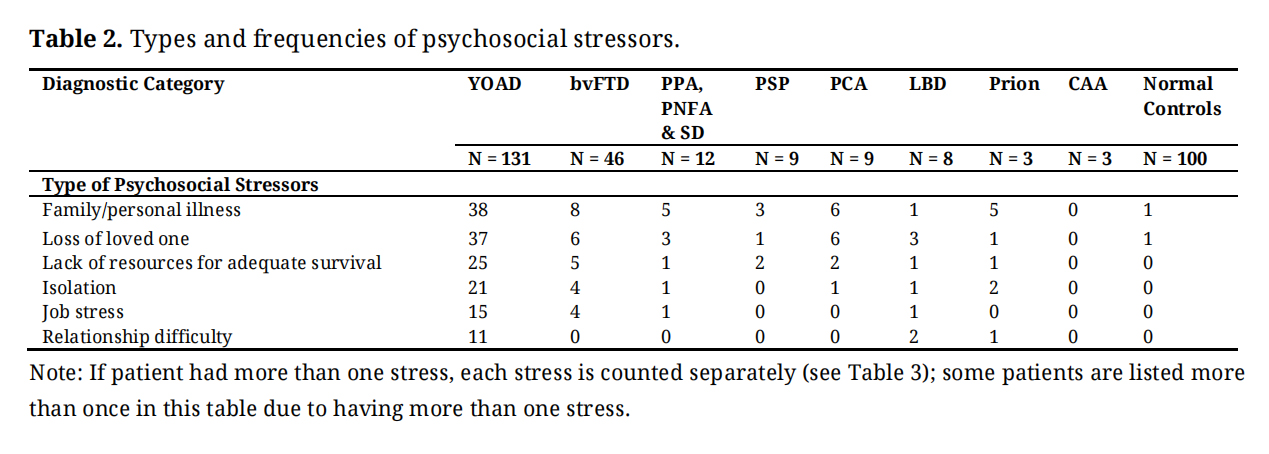 Table 2. Types and frequencies of psychosocial stressors.
Table 2. Types and frequencies of psychosocial stressors.
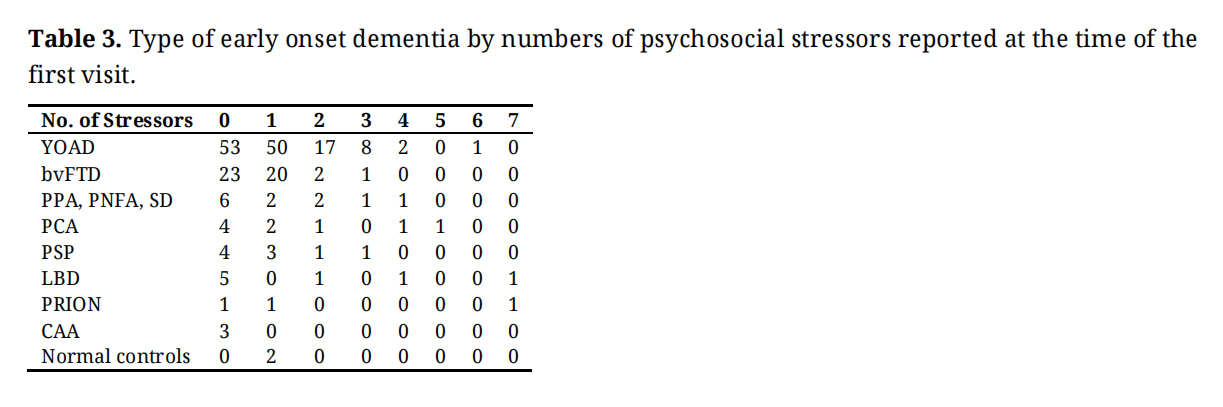 Table 3. Type of early onset dementia by numbers of psychosocial stressors reported at the time of the first visit.
Table 3. Type of early onset dementia by numbers of psychosocial stressors reported at the time of the first visit.
The principal discovery from our investigation was that psychosocial stressors are potential risk factors for YOD. This supports emerging awareness that chronic stress and genetic factors may operate through thalamic, hypothalamic and pituitary mechanisms and the immune system, resulting in neuroinflammation and neurodegeneration [13,14]. Sexual assault in women escalates, not only an increased risk of dementia, but also an increased risk of stroke [15]. We did not identify increased levels of stress in normal controls.
PTSD has been associated with a doubling of dementia risk [16], supporting the concept that traumatic experiences impact brain health [17]. Interestingly, we did not identify many patients with PTSD in our cohort. Depression and anxiety have been related to earlier onset AD, with more than one psychiatric diagnosis resulting in even earlier onset [18].
A Swedish study investigated chronic stress in about 1.3 million people and found an odds ratio of 2.45 of AD in those with chronic stress, 2.32 with depression and 4.00 with chronic stress and depression [10]. A Danish study of about 100,000 people identified a 2.20 higher rate of dementia in those with any stress diagnosis in midlife, compared to those without stress [11]. A Finnish study used self-reported symptoms of psychological distress—like our study—in around 70,000 participants followed over 25 years with elevated incidence ratios of 1.24 for stress with a hazard ratio of 1.12 [19].
Not all the studies have found a relationship between stress and dementia, with one study in amnestic cognitive impairment showing no relationship to the development of dementia, possibly related to a low cortisol level [20]. A prospective study of around 1000 individuals identified a relationship between distress, using a neuroticism scale, with a risk of mild cognitive impairment increasing by 2%; for each unit of increased distress, a distress-prone person was 40% more likely to develop mild cognitive impairment [21].
A Norwegian investigation confirmed distress was associated with increased dementia risk with a hazard ratio of 1.3 in individuals 30–60 years of age and that moderate to vigorous exercise reduced dementia risk in those distressed, compared to those not distressed [22]. A 27-year follow-up study (HUNT1) followed patients for 27 years and recorded self-reported mental distress and showed around 50% increased odds for dementia, reporting that midlife mental stress increased dementia [23]. These studies concentrated on all causes of dementia in large aging populations, whereas our studies concentrate on a small cohort of YOD patients where the diagnoses are segregated and support the notion that self-reported psychosocial risk factors are associated with YOD. Furthermore, perceived stress was associated with a 30% increase in the incidence of amnestic mild cognitive impairment [24]. Also long-term depression has been associated with advancing brain aging, suggesting that stress and depression may accelerate brain aging and neuro-degeneration [25]. Stress related disorders have been linked to future neurodegenerative disorders in a study of over 60,000 people in Sweden and revealed an association between stress and neurodegenerative disorders (HR 1.6), vascular neurodegenerative conditions (HR 1.8), AD (1.4), but not for Parkinson’s disease nor amyotrophic lateral sclerosis [26].
Our study is distinct from these large cohort studies and targets a well-defined group of YOD patients in Perth, Western Australia, and reveals an association between psychosocial stress and neurodegenerative disorders. Psychological studies reveal 35% of Australians have significant stress in their lives; a figure which is now probably higher given the current economic challenges, with 26% having moderate to extremely severe depression [27]. The top five causes of stress in Australia in recent times are financial, family, personal health, trying to maintain a healthy lifestyle and the health of those around us.
A study of almost 25,000 individuals found perceived stress in black and white participants 1.37 odds for poor cognition after adjustment of sociodemographic and other variables and increased prevalence and incidence of cognitive impairment [28]. A systemic review and in-depth analysis supported the idea that perceived psychological stress in adulthood is associated with an increased risk of dementia and mild cognitive impairment [29]. Additionally, memory may be vulnerable to high levels of perceived stress and neuroticism, which is related to stress susceptibility [30].
Enquiries into psychosocial stressors in 800 women found a relationship between long-standing stress and dementia incidence over 38 years from mid- to late-life; the number of psychological stressors was related to dementia incidence four decades later, and the number of psychosocial stressors and AD was independent of perceived distress [31].
AD is distinguished by the deposition of Aβ, phosphorylated tau and neuronal loss; FTD by neuronal loss plus accumulation of tau, but other proteins—like progranulin, TAR DNA-binding protein 43 (TDP-43), C9orf72, fused sarcoma virus and ubiquitin—may also be involved. The physico-chemical responses to stress promoting protein deposition, misfolding and neurodegeneration with neuronal loss, which is fundamental, and irrespective of the proteins involved. The stress pathways advance neurodegenerative processes and are considered foundational and probably relevant to all neurodegenerative operations, and possibly represent a corrective mechanism. Even though we did not see statistical significance in neurodegeneration involving alpha-synuclein and prion proteins, this might be because of the small numbers involved and larger studies with these disorders are required.
Our work suggests an association between perceived psychosocial stress and the development of YOD. To our knowledge, this is the first study of its type and is consistent with larger cohort studies in older populations of the role of stress in dementia.
Our work raises the hypothesis that in vulnerable individuals, psychosocial stressors may be associated with the onset of neurodegenerative disorders in young adults. Our work is observational and has limitations in terms of causality, but does question adult management of psychosocial stress in young adults as a means of minimizing dementia risk and perhaps should be regarded as a modifying risk factor for dementia—and an important take-home from this study.
Mechanistically neural, endocrine and immune pathways respond to stress and, in appropriate individuals (e.g., APOE4 homozygosity) [32], may trigger the neurodegenerative reactions [6]. The endocrine system through the action of glucocorticoids, cytokines, inflammatory and immune interactions with tau, amyloid and other proteins combined with the microglial response resulting in neurodegeneration [33,34]; these interactions driving the amyloidogenic pathway in YOAD. Also more recent studies support an association between psychosocial stress and dementia risk [35].
Psychosocial stress has also been associated with increased risk of stroke [36], and stroke-neurodegeneration interface representing an important area for preventative research.
The limitations of our study are the small numbers and self-reports of stress. Nevertheless, our work in well-defined sporadic YOD patients, their investigation and management by a stable team over many years gives credence to our discovery. It is possible that YOD patients may have a biased recollection of stress in their lives. This is, however, refuted as no increase in stress was found in normal subjects and controls of old onset dementia people. Retrospective self-reports may be misty but often a self-report may be the only way to garner sensitive details about a person’s life stressors—which are subjective. Such bias was averted by establishing stability of the perceived stress over time and ratified by close family. YOD is not a common disease with a prevalence of about 120/100,000 [37]. We have captured most of the patients in Perth, Western Australia, in our study. The N-numbers in our study compare favorably with other non-epidemiological studies of YOD [38]. The N-numbers in our main diagnostic groups (YOAD, FTD) allow a strong statistical analysis in comparison with our control populations.
We recognize there are problems with people recalling information from their previous life and that this might have influenced the outcome of our research. However, we have tried to minimize recall bias by asking our patients at first presentation about their perceived stressors, as well as asking their accompanying family with the patients absent. Furthermore, we confirmed stability of the perceived stress with time and our age-matched normal controls, where the information was collected in the same way and reported minimal psychosocial stress, supporting our conclusions.
To our knowledge there are no systematized measures of stress intensity or duration. The method of detecting stress used in this study relies on the patient and caregiver and must have been a perceived stable stress for at least 6-months. We believe this supports the powerful magnitude and stability of the stress which allows investigation and invites replicability.
We realize the absence of blinding in our study but assessment of stress was made at first contact without knowledge of the diagnosis and confirmed at follow-up, adding soundness to our findings. Our cognitive raters confirmed the stress and assessed the patients unaware of their diagnoses. Our previous studies on this group of patients have not revealed socio-economic or comorbidity differences between the diagnostic populations and controls [1].
With the abundance of biomarkers, subsequent studies may yield fruitful results. Patients with the suspicion of YOD who report psychosocial stressors, measurement of stress markers—like cortisol, pro-inflammatory cytokines such as interleukin-6, metabolic markers namely glucose and a physiological marker (specifically heart rate variability)—might identify a cohort of patients in whom measurement of pTau 217, supporting AD pathology, may be incorporated into studies where treatment of stress with cognitive behavioral therapy or medications (e.g., SSRI inhibitors) might reveal a reduction in dementia frequency in comparison to controls. Young adults reporting psychosocial stress might benefit from appropriate psychological support if identified early to prevent neurodegeneration, particularly if there is a family history of neurodegeneration and a positive neurodegenerative biomarker.
The inferences from our study are twofold: (i) clinically, to carefully support and manage psychosocial stress in young adults with mental health interventions as a means of preventing dementia; and (ii) research, to investigate the role of behavioral and pharmacological means of minimizing stress reactions in young adults in those with biomarker evidence of dementia risk.
The study was approved by the Ethics Committee of Joondalup Health Campus (protocol approval: JHC HREC ARTEMIS 1406).
Regarding the Informed Consent Statement, written informed consent was obtained from all subjects involved in the study.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Table S1: Types of psychosocial stressors.
All data generated from the study are available in the manuscript or supplementary table.
Conceptualization, PKP; Methodology, PKP; Software, H-YC; Validation, H-YC; Formal Analysis, H-YC; Investigation, PKP; Resources, PKP; Data Curation, PKP; Writing—Original Draft Preparation, PKP; Writing—Review & Editing, PKP; Visualization, PKP; Supervision, PKP; Project Administration, PKP.
The authors declare that they have no conflicts of interest.
This research was supported by Neurodegenerative Disorders Research Pty Ltd; no external funding was received.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
Panegyres PK, Chen H-Y. Psychosocial stress as a potential risk factor for young onset dementia. J Psychiatry Brain Sci. 2025;10(4):e250011. https://doi.org/10.20900/jpbs.20250011.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




