Location: Home >> Detail
J Psychiatry Brain Sci. 2026;11(3):e260010. https://doi.org/10.20900/jpbs.20260010
 ,
Shannen Kyte 1,2 ,
Nivashi Arulventh 3 ,
Mahwish Ali Khan 4 ,
Hana Abbasian 5 ,
Zahra Wakif 2,6 ,
Aaima Akbar Cheema 1,2,7 ,
Ruchi Raiker 8,9 ,
Sophia Khan 10 ,
Fatima Nadeem 11 ,
Muhammad Ayub 12 ,
Farooq Naeem 2,13 ,
,
Shannen Kyte 1,2 ,
Nivashi Arulventh 3 ,
Mahwish Ali Khan 4 ,
Hana Abbasian 5 ,
Zahra Wakif 2,6 ,
Aaima Akbar Cheema 1,2,7 ,
Ruchi Raiker 8,9 ,
Sophia Khan 10 ,
Fatima Nadeem 11 ,
Muhammad Ayub 12 ,
Farooq Naeem 2,13 ,
1
2
3
4
5
6
7
8
9
10
11
12
13
*
Background: Depression and anxiety are highly prevalent among South Asian populations, yet the effectiveness of cognitive behavioural therapy (CBT), including culturally adapted approaches, has not been comprehensively synthesized. This study aimed to evaluate the efficacy of CBT in reducing depressive and anxiety symptoms among South Asian adults. Methods: A systematic review and meta-analysis were conducted in accordance with PRISMA guidelines and registered in PROSPERO (CRD42025631254). Electronic databases were searched through February 2024 for randomized controlled trials examining CBT interventions among South Asian adults in both South Asian and diaspora settings. Sixteen trials met the inclusion criteria. Effect sizes were calculated using Hedges’ g within random-effects models. Between-study heterogeneity was quantified using the I2 statistic, and publication bias was assessed using funnel plots, Egger’s regression test, and trim-and-fill analyses. Results: Across 3158 participants, CBT was associated with significant reductions in depressive symptoms (g = −1.30, 95% CI [−2.14, −0.45], p = 0.003) and anxiety symptoms (g = −1.28, 95% CI [−1.87, −0.69], p < 0.001). Improvements were also observed in disability and quality-of-life outcomes. However, substantial heterogeneity was detected (I2 > 90% for depression and anxiety), indicating variability in treatment effects across contexts and intervention formats. Adjusted analyses suggested that pooled effects remained statistically significant. Conclusions: CBT, including culturally adapted interventions, demonstrates potential effectiveness for reducing depression and anxiety among South Asian adults. Nonetheless, substantial heterogeneity and potential small-study effects highlight the need for cautious interpretation and further research into contextual and cultural moderators of treatment response.
BaCBT, Adapted Bengali Cognitive Behavioural Therapy; CaCBT, Culturally-Adapted Cognitive Behavioural Therapy; BA-M, Behavioural Activation Therapy adapted for Muslims; CBT, Cognitive Behavioural Therapy; C-MAP, Culturally adapted Manual-Assisted Problem-solving therapy; LTP, Learning Through Play; CA-CBT+, Culturally-Adapted Cognitive Behavioural Therapy + Problem Solving; CatCBT GSH, Culturally-adapted trauma-focused Cognitive Behavioural Therapy-based Guided Self-Help; CaCBT-GSH, Culturally-adapted Cognitive Behavioural Therapy-based Guided Self-Help; HAP, Healthy Activity Program; bCBT, Brief Cognitive Behavioural Therapy; TAU, Treatment as Usual; THP, Thinking Healthy Programme; bCBGT, Brief Cognitive Behavioural Group Therapy; CA-CBT, Culturally Adapted Cognitive-Behavioural Therapy; THPP, Thinking Healthy Programme Peer-delivered; RCT, Randomized Controlled Trial; OCD, Obsessive Compulsive Disorder; PTSD, Post-Traumatic Stress Disorder; GAD, Generalized Anxiety Disorder; CBGT, Cognitive Behavioural Group Therapy; DS, Depression Scale; Y-BCOS, Yale-Brown Obsessive Compulsive Disorder Scale; HADS, Hospital Anxiety & Depression Scale; CAPS, Clinician-Administered PTSD Scale; PCL, PTSD Checklist; DAS, Dyadic Adjustment Scale; PHQ-9, Patient Health Questionnaire-9; DUOCS, Dhaka University Obsessive Compulsive Scale; BSS, Beck Scale for Suicidal Ideation; HDRS, Hamilton Depression Rating Scale; EPDS, Edinburgh Postnatal Depression Scale; GHQ-28, General Health Questionnaire-28; SUS, System Usability Scale; TSAM, Treatment Satisfaction and Acceptability Measure; AD, Aga Khan Anxiety and Depression Scale; HITS, Hurt, Insulted, Threatened with harm, Screamed at them; GAD-Q-IV, Generalized Anxiety Disorder Questionnaire Fourth Edition; LSAS, Liebowitz Social Anxiety Scale; SIAS, Social Interaction Anxiety Scale; CES-D, Center for Epidemiological Studies Depression Scale; RHS-15, Refugee Health Screener 15; HSCL-25, Hopkins Symptom Checklist 25; HTQ, Harvard Trauma Questionnaire
Depression and anxiety are major contributors to the global disease burden [1]. The occurrence of these conditions has increased, with one in five individuals experiencing depressive or anxiety disorders during their lifetime [2]. These conditions often co-occur with other illnesses, which lead to significant lifelong impairments [3,4]. While psychological treatments are becoming more accessible, substantial gaps in access to evidence-based mental health care remain, particularly in low- and middle-income countries (LMICs), where approximately 80% of people with mental disorders live [5,6]. Limited infrastructure, a shortage of trained providers, cultural beliefs, stigma, and other contextual barriers further reduce treatment availability and engagement in these areas [6,7]. This disparity underscores the urgency of equitable, contextually relevant interventions applicable across diverse healthcare settings [1,8].
Among South Asian populations, individuals experience elevated vulnerability to depression and anxiety due to distinct sociocultural and structural factors. These vulnerabilities are shaped by sociocultural factors such as stigma, family dynamics, explanatory models of illness, and barriers to help-seeking [9,10]. South Asian communities often follow a collectivistic social structure. Family involvement, religious beliefs, and community norms are central tenets of mental health experiences, including symptom expression and pathways to care [11,12]. These factors are associated with delayed help-seeking behaviour, underutilization of formal mental health services, and inconsistent engagement in psychological treatments [8,13]. Sociocultural factors, such as migration-related stressors and structural barriers, play a central role in forming mental health experiences and engagement with care [12,13].
Cognitive behavioural therapy (CBT) is a well-known, first-line treatment for depression and anxiety, with substantial evidence illustrating its effectiveness across clinical settings [14–17]. However, its traditional structure and content were developed within Western cultural contexts, ideas, and values. As a result, standard CBT may not fully reflect the cultural norms, illness beliefs, communication methods, and family dynamics common among South Asian populations [18,19]. Therefore, culturally adapted CBT (CaCBT) interventions were developed to incorporate linguistic, religious, and diverse sociocultural considerations specific to South Asian settings [19,20]. Across South Asian settings, CBT and CaCBT interventions have been implemented through diverse formats, including individual- and group-based approaches and community-oriented models, to improve accessibility and acceptability [20,21]. Early trials show favourable acceptability and symptom improvement among South Asian populations in both their countries of origin and diaspora settings [22,23].
Although these encouraging results are promising, evidence for CaCBT in South Asian populations remains fragmented, comprising feasibility studies, small randomized controlled trials, and community-based interventions [19,22,23]. Previous meta-analyses of psychosocial interventions in non-Western contexts have highlighted significant methodological variability, including diverse diagnostic groups, brief follow-up periods, and inconsistent frameworks for adaptation. These factors hinder the clear interpretation and practical use of combined data [18]. Consequently, the overall effect of CBT for depression and anxiety among South Asian adults has not been clearly quantified [18,20]. This review aims to integrate data from randomized controlled trials regarding the efficacy of Cognitive Behavioural Therapy (CBT), including its variations across different intervention subtypes, for the treatment of depression and anxiety within South Asian populations.
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [24] and was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42025631254. Ethical approval was not required for this study, as it involved secondary analysis of data from previously published studies and did not include individual-level participant data.
Search StrategyThe search strategy was developed by a medical librarian following the Peer Review of Electronic Search Strategies (PRESS) 2015 Guidelines [25]. Searches were conducted across PsycINFO, MEDLINE, Embase, CINAHL, Web of Science, Cochrane Library, and Index Islamicus. The initial search was conducted in June 2020 and identified 156 records, of which 9 studies met the final inclusion criteria. The search was updated in February 2024. This updated search yielded 715 records in total, including overlap with records identified in the original 2020 search. After deduplication across the combined search set, 535 unique records remained for title and abstract screening. The updated screening process contributed 7 additional eligible studies, resulting in a total of 16 included randomized controlled trials.
Both controlled vocabulary (e.g., MeSH terms and the Thesaurus of Psychological Index Terms) and free-text keywords were used to identify studies. Searches were limited to English-language, adult human studies and encompassed a range of CBT modalities, including acceptance and commitment therapy, dialectical behaviour therapy, mindfulness-based interventions, and behavioural activation. These modalities were included because they share core cognitive-behavioural theoretical foundations and are frequently grouped within the broader CBT literature. However, they differ in theoretical emphasis and clinical application, which may contribute to heterogeneity between studies (see Limitations). The reference lists of included articles were manually screened to identify additional eligible studies. Complete database-specific search strings are presented in Flie S1.
Eligibility CriteriaTo be included in this systematic review and meta-analysis, studies were required to meet several specific criteria. First, the population had to consist of South Asian adults aged 16 or older, originating from Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, Sri Lanka, or the South Asian diaspora. There was no restriction for inclusion by country of residence, as culturally adapted CBT targets culturally shaped beliefs, stigma, family roles, and help-seeking practices that may remain vital among South Asian diaspora communities [18,19]. Accordingly, trials conducted in Western countries were deemed eligible where participants were explicitly identified as South Asian, and the intervention addressed culturally relevant barriers or preferences.
These individuals needed to have symptoms of, or a diagnosis of, depression, anxiety disorders, phobias, obsessive-compulsive disorder (OCD), or post-traumatic stress disorder (PTSD), as defined by the DSM-IV-TR, DSM-V, or ICD-11 diagnostic criteria. Although several internalizing diagnoses were eligible at screening, the primary outcomes for quantitative synthesis were depression and anxiety symptom measures; trials involving OCD or PTSD were included only where depression and/or anxiety outcomes were reported and were otherwise summarized descriptively. The studies were also required to evaluate interventions using CBT, either delivered in individual or group settings. Additionally, studies using any form of CBT, including its subtypes such as mindfulness-based CBT or behavioural activation, were considered for inclusion. Eligible studies had to use a randomized controlled trial (RCT) design, with both pre- and post-intervention measurements and comparisons with no intervention, a placebo, or other active interventions. Cultural adaptation of CBT was not an inclusion criterion, but studies explicitly describing culturally adapted protocols were noted descriptively.
Participants with active suicidal ideation or recent self-harm were excluded to align with current clinical guidelines that prioritize urgent risk assessment and crisis-oriented management over standard CBT protocols [26]. Likewise, individuals with current or recent substance use disorders (SUDs) were excluded as SUDs independently influence mood and/or anxiety outcomes and are often treated using distinct CBT subtypes; in antidepressant and related trials, SUDs are among the most frequently applied exclusion criteria [26]. Only studies published in English and appearing in peer-reviewed journals were included in the review. Studies were excluded if they involved participants under the age of 16, individuals diagnosed with psychotic disorders, or those that focused primarily on physical health comorbidities rather than mental health conditions. This exclusion criterion ensured the review focused on non-crisis outpatient populations, consistent with standard eligibility practices.
Screening ProcedureThe screening process for this systematic review was conducted in two distinct phases after the search results were imported into Covidence [27], a systematic review management software. First, the software automatically identified and excluded duplicates. The screening then proceeded in two phases: title and abstract screening, followed by full-text screening.
In the initial phase, all investigators screened the first 100 titles and abstracts together with the research lead (VI) and supervisor (FN) for training purposes. This step ensured that all reviewers agreed with the decisions made in the first 100 screenings and were aligned in their understanding and application of the inclusion and exclusion criteria. There were 4 reviewers for the screening process who were familiar with the review proposal and screening guidelines and who had received an undergraduate degree or higher. Once consistency was established, the remaining titles and abstracts were independently screened by two reviewers. The reviewers worked in pairs to determine whether each study should be included or excluded based on the predefined eligibility criteria. Specific reasons for excluding studies were meticulously documented at this stage. Importantly, author names were not blinded to enable a more transparent review process.
Any disagreements between the two reviewers regarding the inclusion or exclusion of studies were resolved through weekly meetings, facilitated by the research lead (VI) and supervisor (FN). During these meetings, discussions were held to reach a consensus on any unclear articles. Having two independent reviewers assess each study significantly reduced the risk of bias and ensured that the screening process remained rigorous and objective. Once the studies met the inclusion criteria, they advanced to the data extraction stage for further analysis. This multi-step approach helped maintain a high level of reliability and consistency throughout the screening process.
Data Extraction ProcessThe data extraction process was guided by a pre-designed form based on the Cochrane Handbook [28]. This form was used by all reviewers to collect consistent information from each study, ensuring comprehensive and comparable extraction across all studies included in the review. The form captured details such as population characteristics, study design, methods used for intervention and control groups, risk of bias, primary outcome measures, and study limitations (See Flie S2 for the form).
Before the official review commenced, a calibration exercise was performed to ensure consistency and reliability among all reviewers. Each researcher completed two pilot data extractions using the same article, and any discrepancies in the extraction process were discussed and resolved to ensure alignment of the team’s approach. Throughout the data extraction phase, the research supervisor (FN) and the lead investigator (VI) provided weekly supervision to maintain consistency and address any emerging issues.
Data extraction for this systematic review was conducted by the research team (VI, SK, NA, and MA) using a standardized, structured approach. The extraction process focused on several key variables, including demographic details (age, sex, and country of study); the study design; the type of CBT sessions (individual or group); and the instruments used to measure mental health outcomes. The outcomes assessed included symptoms of major depressive disorder (MDD), generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD), phobias, and post-traumatic stress disorder (PTSD). In addition to these, data were also collected on the study population, setting, methods, risk of bias, intervention and control groups, primary outcome measures, process variables, applicability, limitations, and critical conclusions drawn from each study.
To assess the quality of the included studies, the Cochrane Risk of Bias tool [29] was used. This tool evaluates seven domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. Each domain was rated as low, high, or unclear risk of bias. Risk-of-bias assessments were initially completed by one reviewer and independently validated by a second reviewer. Any discrepancies identified during the validation process were discussed and resolved through consensus. Study-level bias was rated as high if any individual domain was rated high risk or if two or more domains were rated as unclear risk.
Data AnalysisWe used a random-effects model to examine outcomes, accounting for variation in observed intervention effects due to inherent differences and sampling variability. This model is appropriate as it accounts for heterogeneity across studies. Statistical analyses were conducted using R Statistical Software (version 4.4.1) [30] and the metafor package (version 4.6-0) [31]. The analyses were conducted under the expert guidance of MA, a meta-analysis specialist, ensuring the precise and reliable application of statistical methods. Sample characteristics, including race, age, and sex, derived from descriptive statistics provided insight into the diversity and representativeness of the study samples.
The primary analyses focused on assessing the effectiveness of CBT in improving mental health symptoms of anxiety and depression among South Asian populations and their diaspora. Additional psychosocial outcomes, including disability, quality of life (QOL), and social support, were also documented for future analysis. PTSD outcomes were summarized descriptively and were not included in quantitative synthesis. We used a random-effects model for analysis because we anticipated heterogeneity across studies. We used the standardized mean difference as the outcome because studies used different symptom scales. According to Cohen’s guidelines, effect sizes are classified as small (0.2), medium (0.5), and large (0.8) [32].
Between-study heterogeneity was quantified using the I² statistic, which estimates the proportion of total variability attributable to between-study heterogeneity rather than sampling error [33]. Random-effects models were fitted using the DerSimonian and Laird method. This approach complements the random-effects model by accounting for variability in study outcomes stemming from differences in study populations, interventions, and methodologies.
We used the Egger test to assess publication bias. This was assessed by examining asymmetry in funnel plots. Funnel plots were created to visualize the distribution of study effect sizes and standard errors. In cases where the Egger’s test indicated a publication bias, suggesting that smaller studies with non-significant results might be missing, we applied the trim-and-fill method to estimate and adjust the summary effect size [34]. This method computes the pooled effect size by imputing data from missing studies.
When studies reported multiple measures of the same outcome (e.g., multiple anxiety scales or quality-of-life domains), all eligible measures were extracted and included as separate effect sizes within outcome-specific analyses. Because effect sizes derived from the same sample may be statistically dependent, pooled estimates should be interpreted cautiously, as this approach may underestimate standard errors and overstate precision.
More advanced methods such as multilevel meta-analysis or robust variance estimation, were not implemented, as the proportion of studies contributing multiple effect sizes was small and the pre-specified analysis plan did not include these techniques. This limitation is discussed further in the Limitations section.
Formal subgroup analyses by CBT intervention type were not conducted. While the inclusion of diverse CBT modalities (standard CBT, k = 3; culturally adapted CBT, k = 8; CBT elements, k = 5) likely contributed to between-study heterogeneity, the small number of studies within each category precluded reliable subgroup comparisons. Findings are discussed qualitatively by intervention type, country, delivery format, and clinical population in the Discussion section.
Primary analyses focused on post-intervention outcomes. Follow-up assessments were not synthesized due to variability in follow-up timing and inconsistent reporting across studies (see Limitations).
Forest plots were used to illustrate the effect sizes of individual studies and the overall pooled effect, offering a visual representation of the consistency of results across studies. Both funnel and forest plots were instrumental in further exploring potential bias. Where necessary, trim-and-fill analyses were also conducted for each funnel plot to yield adjusted effect sizes that account for potential publication bias.
Figure 1 presents the PRISMA flow diagram summarizing the study selection process. A total of 715 records were identified through database searches, and 180 duplicates were removed, leaving 535 records for title and abstract screening. Of these, 264 records were excluded. Reports were sought for retrieval for 271 records; 102 reports were not retrieved, and 169 full-text reports were assessed for eligibility. Following full-text review, 153 reports were excluded for reasons including ineligible outcomes, study design, population, or intervention characteristics. Sixteen randomized controlled trials met the inclusion criteria and were included in the final review. Detailed study characteristics are provided in Table 1.
Sixteen randomized controlled trials met the inclusion criteria (Figure 1). Across the included studies, 1612 participants were allocated to intervention groups and 1546 to control groups, yielding a total sample of 3158 participants. The mean age across studies ranged from 19.2 to 48.63 years, with standard deviations ranging from 0.55 to 13.0. All participants were of South Asian origin. Studies were conducted in Pakistan (n = 9), India (n = 5), Bangladesh (n = 1), and the United Kingdom (n = 1). Eight interventions were explicitly described as culturally adapted CBT. Other intervention formats included self-help (n = 3), Thinking Healthy Program (n = 3), behavioural activation (n = 1), group-based interventions (n = 2), brief interventions (n = 3), internet-delivered interventions (n = 1), and integrated approaches (n = 1). Control conditions included treatment as usual (n = 7), waitlist control (n = 3), and active treatment control (n = 6). Intervention duration ranged from 6 weeks to 2 years, with most programs lasting 10–12 weeks (n = 7). Session length varied from 15 to 120 min, with 30–60-min sessions most common (n = 4). Of the 16 studies, approximately 11 reported follow-up assessments beyond the post-intervention time point (ranging from 1 to 12 months), while 5 measured post-intervention outcomes only. See Table 1 for detailed study characteristics.
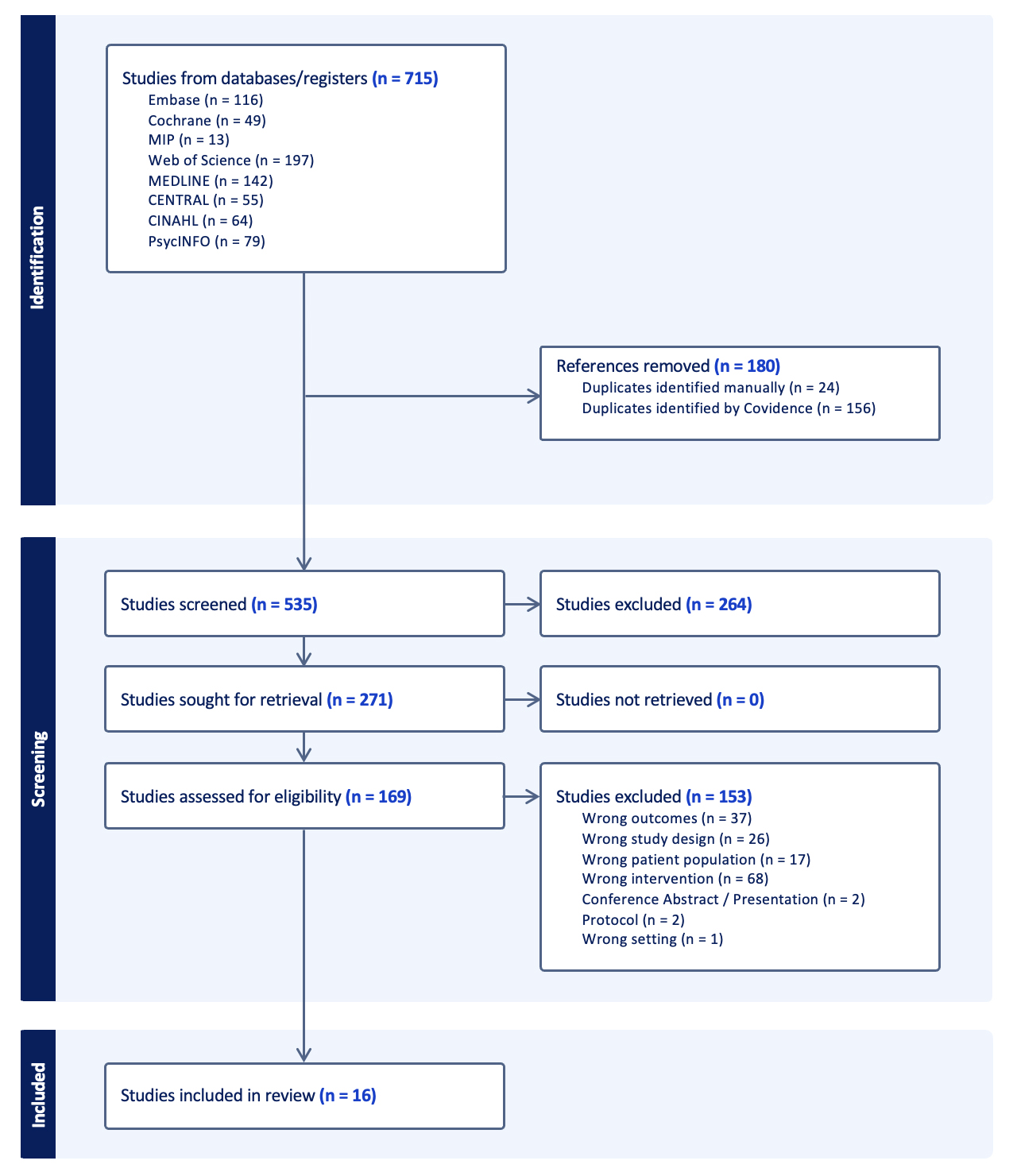 Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Flow Diagram. Note. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flowchart outlining the study selection process.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Flow Diagram. Note. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flowchart outlining the study selection process.
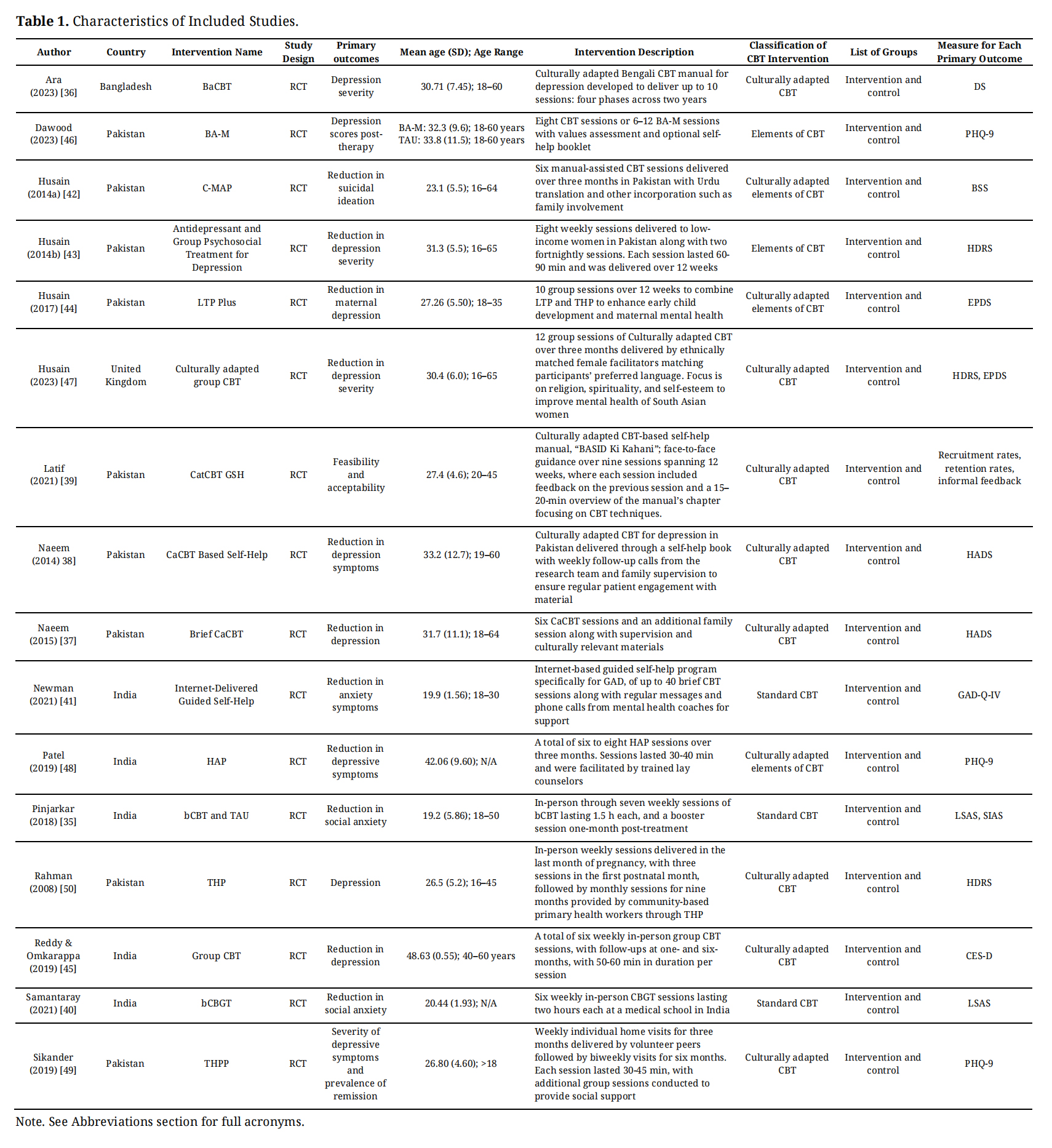 Table 1. Characteristics of Included Studies.
Table 1. Characteristics of Included Studies.
A total of seven studies measured the effects of CBT on anxiety in the South Asian population, with Pinjarkar [35] using two measures of anxiety. There were 413 participants in the treatment group and 398 in the control group, for a final sample of 811. The mean age across studies was approximately 27.0 years, with standard deviations ranging from 1.55 to 11.1 years. All participants included were South Asian. The studies included in this analysis were conducted in various countries, including India (n = 3), Pakistan (n = 3), and Bangladesh (n = 1).
Figure 2 presents a forest plot of anxiety outcomes (k = 8), indicating that CBT effectively reduced anxiety symptoms among South Asian participants, with an overall effect size of g = −1.28 (95% CI [−1.87,−0.69], z = −4.25, p < 0.001). However, there was high heterogeneity among the studies (Q(7) = 73.68, p < 0.0001, τ2 = 0.65, I2 = 92.83%), suggesting variability in the effectiveness of CBT for anxiety in South Asian populations across different contexts and study designs (Figure 2). The Egger’s regression test was used to assess asymmetry in the funnel plot using a linear regression model. The results of Egger’s test (z = −1.90, p = 0.057) did not indicate significant publication bias (Figure 3). However, trim-and-fill analysis identified one study that may be missing on the left side of the funnel, indicated by the white circle in Figure 3. When adjusting for the missing study, the effect size and significance increased to g = −1.43 (95% CI [−2.03,−0.83], p < 0.001).
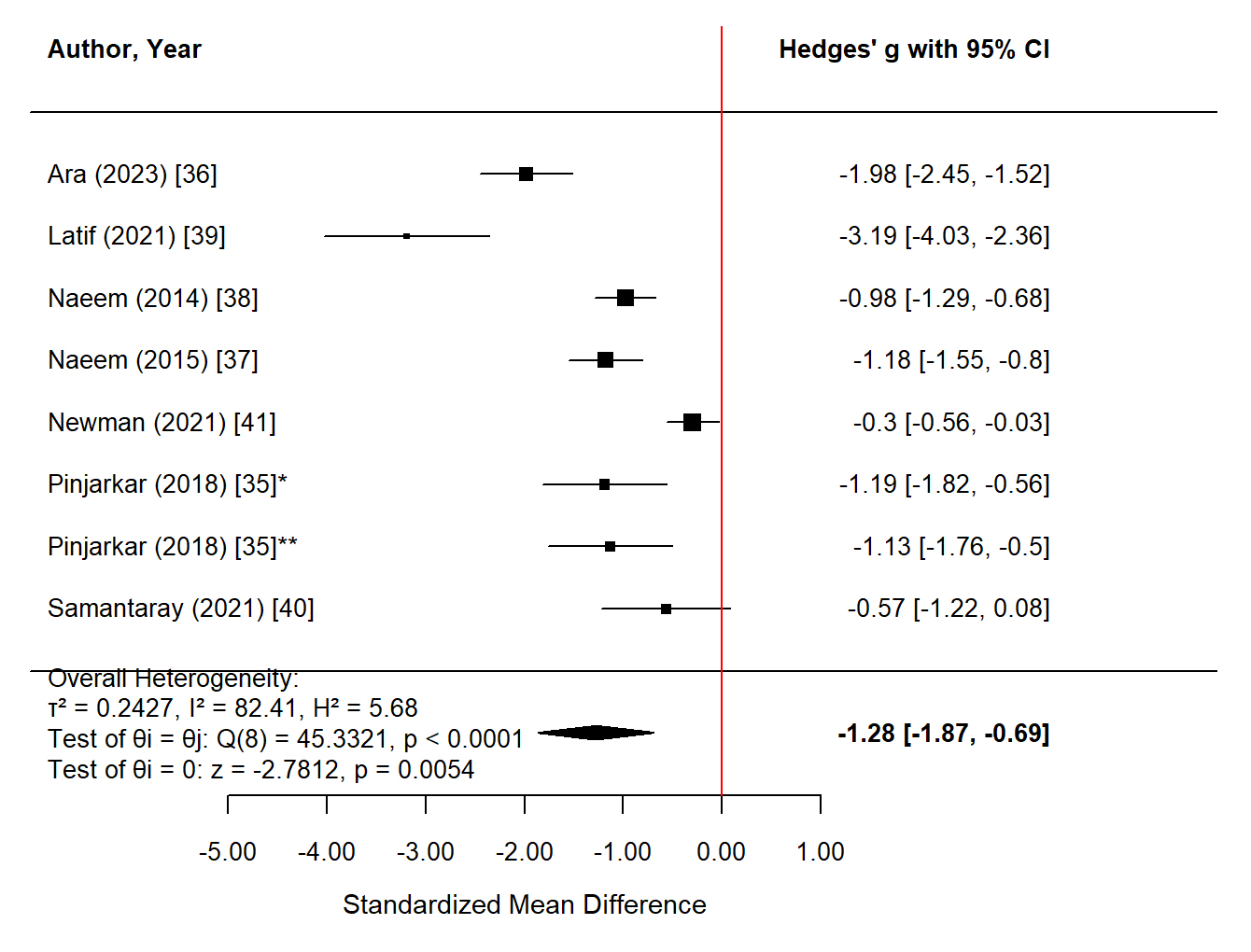 Figure 2.
Forest Plot of the Effect of CBT on Anxiety in the South Asian Population. Note. The following scales were used: Anxiety Scale (AS) [36], Hospital Anxiety and Depression Scale (HADS-Anxiety subscale) [37–39], Liebowitz Social Anxiety Scale (LSAS) [35,40],Social Interaction Anxiety Scale (SIAS) [35], and Generalized Anxiety Disorder Questionnaire (GAD-Q-IV) [41]. *Liebowitz Social Anxiety Scale (LSAS). **Social Interaction and Anxiety Scale (SIAS). The black squares represent individual study effect sizes, with the size of each square proportional to the study weight in the analysis; the black diamond represents the overall pooled effect size from the random-effects model, with its width indicating the 95% confidence interval.
Figure 2.
Forest Plot of the Effect of CBT on Anxiety in the South Asian Population. Note. The following scales were used: Anxiety Scale (AS) [36], Hospital Anxiety and Depression Scale (HADS-Anxiety subscale) [37–39], Liebowitz Social Anxiety Scale (LSAS) [35,40],Social Interaction Anxiety Scale (SIAS) [35], and Generalized Anxiety Disorder Questionnaire (GAD-Q-IV) [41]. *Liebowitz Social Anxiety Scale (LSAS). **Social Interaction and Anxiety Scale (SIAS). The black squares represent individual study effect sizes, with the size of each square proportional to the study weight in the analysis; the black diamond represents the overall pooled effect size from the random-effects model, with its width indicating the 95% confidence interval.
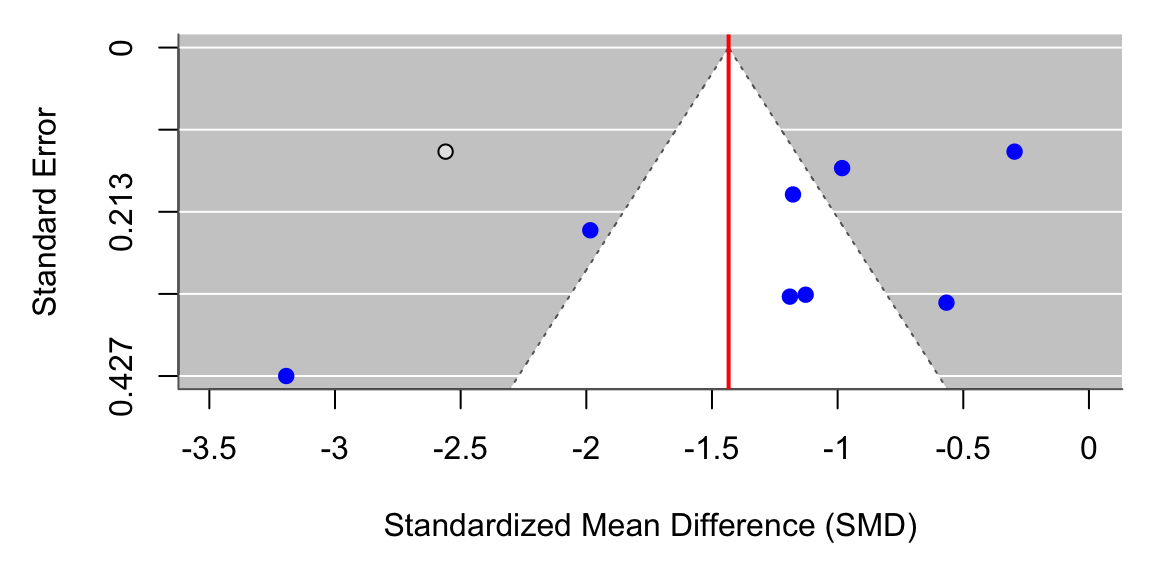 Figure 3.
Adjusted Funnel Plot of the Effect of CBT on Anxiety in the South Asian Population Using a Random-Effect Model Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
Figure 3.
Adjusted Funnel Plot of the Effect of CBT on Anxiety in the South Asian Population Using a Random-Effect Model Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
A total of fifteen studies measured the effects of CBT on depression in the South Asian population. A total of 3108 individuals were included in these studies, with 1587 participants in the treatment group and 1521 in the control group. The mean age across studies was 30.57 years, with standard deviations ranging from 0.55 to 11.1. All participants included were South Asian. The studies included in this analysis were conducted in various countries, including Pakistan (n = 9), India (n = 4), Bangladesh (n = 1), and the United Kingdom (n = 1).
Figure 4 presents a forest plot of depression outcomes (n = 15), showing that CBT was associated with a significant reduction in depressive symptoms among South Asian participants (pooled effect size, g = −1.30; 95% CI [−2.14,−0.45]; p = 0.0026). Substantial heterogeneity was observed across studies (Q(14) = 498.57, p < 0.0001, I2 = 99.18%), indicating considerable variability in treatment effects across study contexts and designs. Funnel plot inspection and Egger’s regression test suggested the presence of publication bias (Figure 5). Trim-and-fill analysis identified two potentially missing studies on the left side of the funnel; after adjustment, the pooled effect size increased to g = −1.49 (95% CI [−2.28,−0.71], p = 0.0002), suggesting that the overall antidepressant effect of CBT remained robust after accounting for small-study effects.
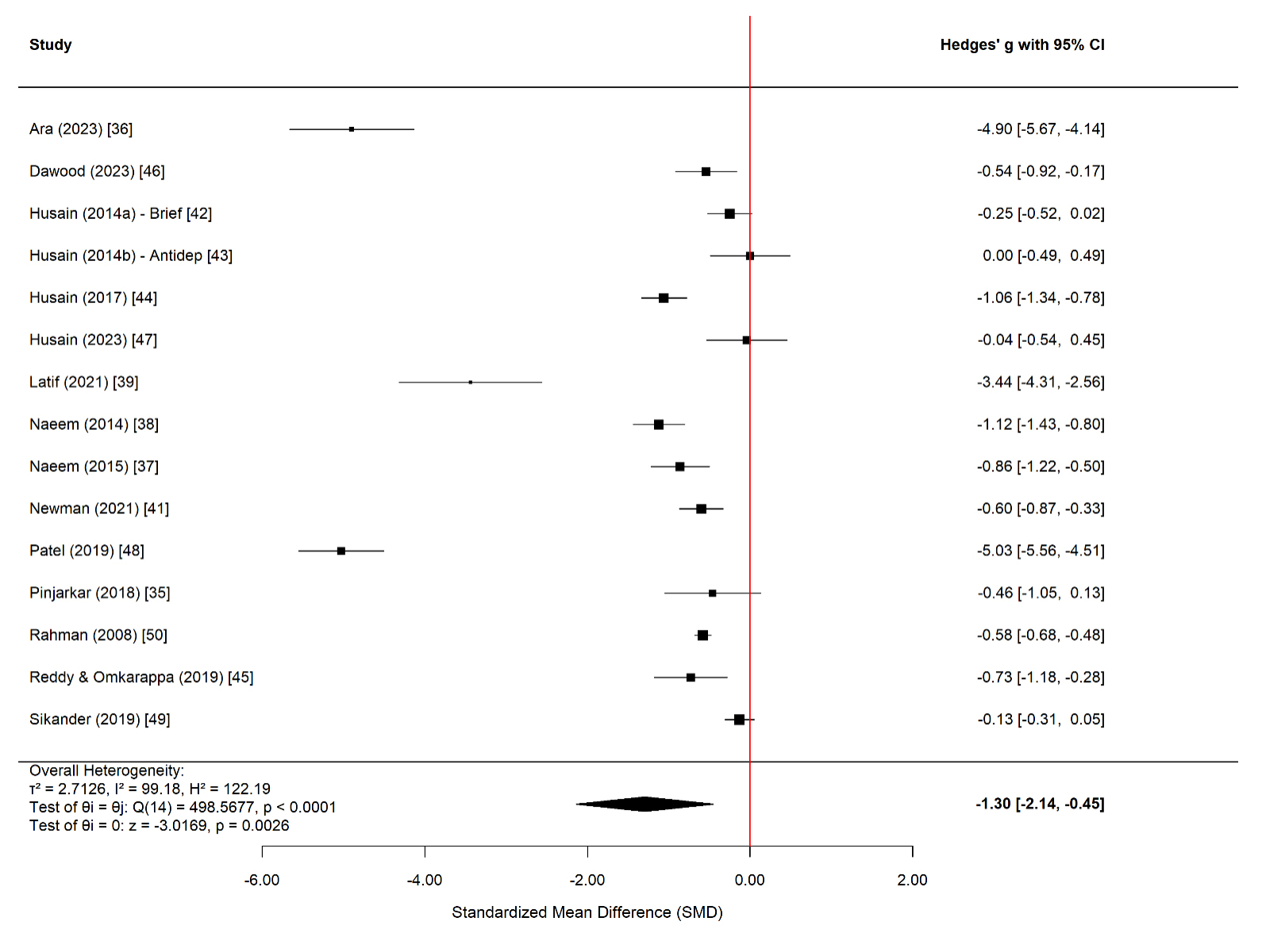 Figure 4.
Forest Plot of the Effect of CBT on Depression in the South Asian Population. Note. The following scales were used: Depression Scale (DS) [36], Hospital Anxiety and Depression Scale (HADS-Depression subscale) [37–39,42–44], Depression Anxiety Stress Scales (DASS-Depression subscale) [41], Beck Depression Inventory-II (BDI-II) [35,45], Patient Health Questionnaire-9 (PHQ-9) [46–49], and Hamilton Depression Rating Scale (HAM-D) [50]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
Figure 4.
Forest Plot of the Effect of CBT on Depression in the South Asian Population. Note. The following scales were used: Depression Scale (DS) [36], Hospital Anxiety and Depression Scale (HADS-Depression subscale) [37–39,42–44], Depression Anxiety Stress Scales (DASS-Depression subscale) [41], Beck Depression Inventory-II (BDI-II) [35,45], Patient Health Questionnaire-9 (PHQ-9) [46–49], and Hamilton Depression Rating Scale (HAM-D) [50]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
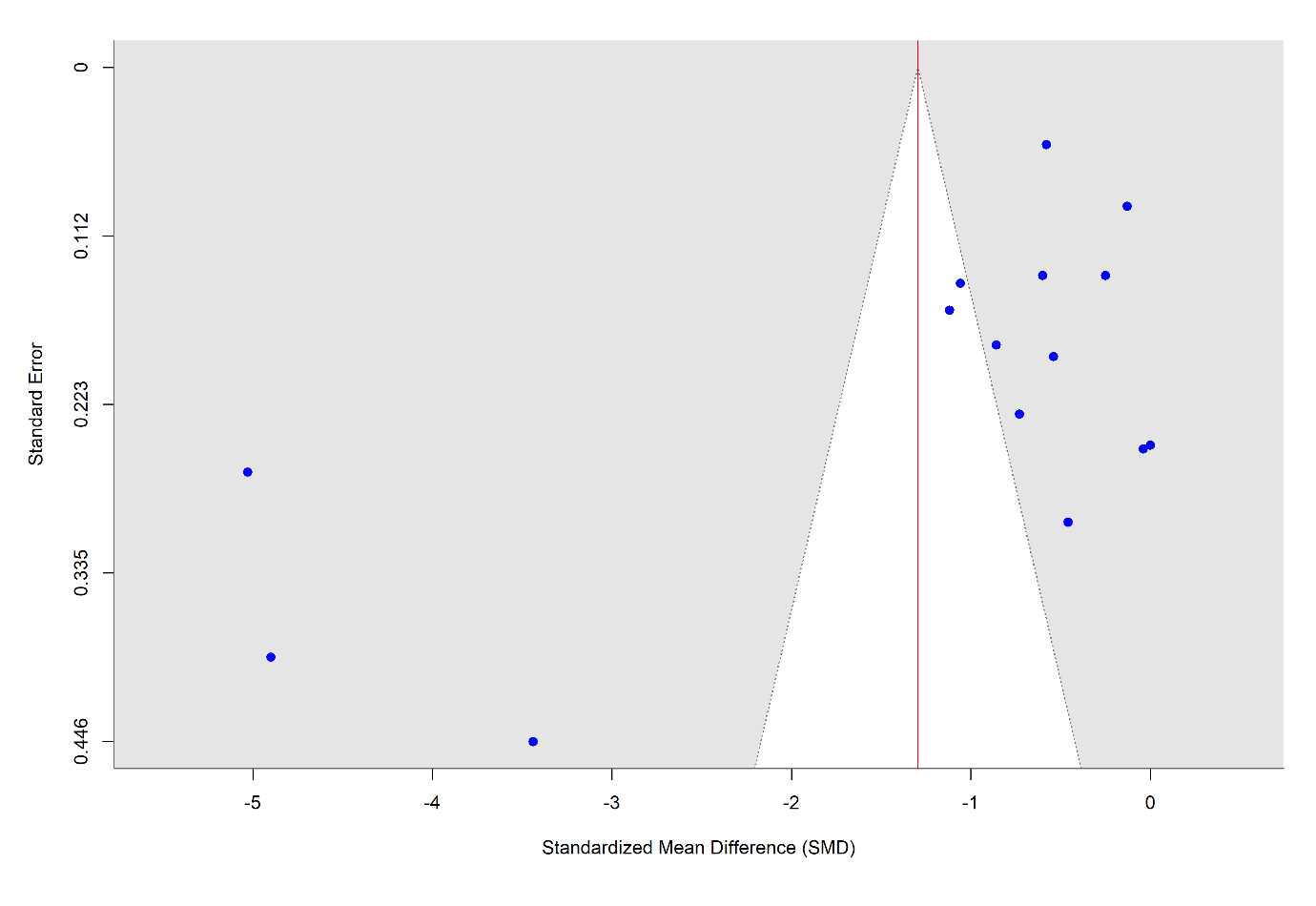 Figure 5.
Adjusted Funnel Plot of the Effect of CBT on Depression in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
Figure 5.
Adjusted Funnel Plot of the Effect of CBT on Depression in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
A total of seven studies measured the effects of CBT on disability in the South Asian population. There were 1092 participants in the treatment group and 1074 in the control group, for a total of 2166. The mean age across studies was 29.166 years, with standard deviations ranging from 4.6 to 11.1. All participants included were South Asian. All the studies included in this analysis were conducted in Pakistan.
Figure 6 presents a forest plot of disability outcomes (n = 7), indicating that CBT was associated with a significant reduction in disability symptoms among South Asian participants (pooled effect size g = −0.83, 95% CI [−1.62, −0.03], p < 0.05). Substantial heterogeneity was observed across studies (Q(6) = 77.64, p = 0.0001, I2 = 98.36%), suggesting considerable variability in effects across study contexts and designs. Funnel plot inspection and Egger’s regression test indicated significant publication bias (Figure 7). Trim-and-fill analysis identified two potentially missing studies on the left side of the funnel; after adjustment, the pooled effect size increased to g = −1.17 (95% CI [−1.92,−0.41], p = 0.003), indicating that the disability-reducing effect of CBT remained robust after accounting for small-study effects.
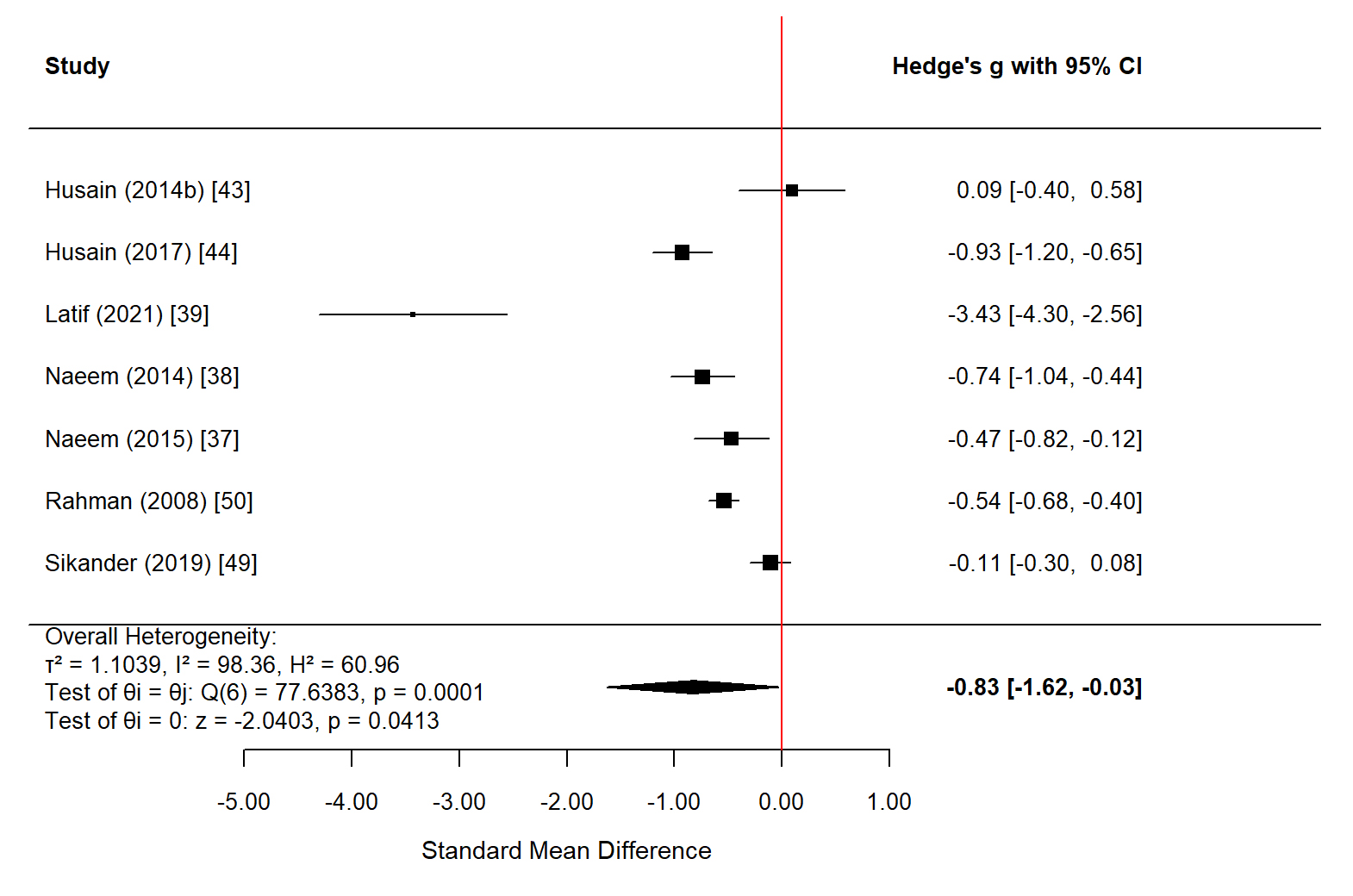 Figure 6.
Forest Plot of the Effect of CBT on Disability in the South Asian Population. Note. The following scales were used: the Brief Disability Questionnaire (BDQ) [37,38,43,44,50] and the WHO Disability Assessment Schedule 2.0 (WHO DAS 2.0) [39,49]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
Figure 6.
Forest Plot of the Effect of CBT on Disability in the South Asian Population. Note. The following scales were used: the Brief Disability Questionnaire (BDQ) [37,38,43,44,50] and the WHO Disability Assessment Schedule 2.0 (WHO DAS 2.0) [39,49]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
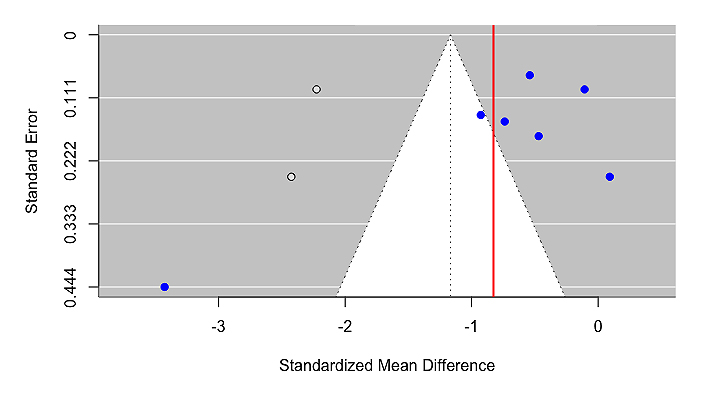 Figure 7.
Adjusted Funnel Plot of the Effect of CBT on Disability in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
Figure 7.
Adjusted Funnel Plot of the Effect of CBT on Disability in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
A total of four studies measured the effects of CBT on quality of life in the South Asian population, with Dawood et al. (2023) [46] including four domains of quality of life. A total of 484 individuals were included in these studies. There were 240 participants in the treatment group and 244 participants in the control group. The mean age across studies was 29.28 years, and the standard deviations ranged from 5.5 to 9.6. All participants included were South Asian. Most of the studies included in this analysis were conducted in Pakistan (n = 3), with one in the United Kingdom (n = 1).
Figure 8 presents a forest plot of quality-of-life outcomes (n = 7), indicating that CBT effectively improved the quality of life in the South Asian population, with an overall effect size of g = 0.33 (95% CI [0.04,0.63], df = 6, p < 0.05). However, considerable heterogeneity was observed among the studies (Q = 19.82, p < 0.01, I2 = 73.68%, df = 6), suggesting variability in the effectiveness of CBT for quality of life across contexts and study designs within South Asian populations (Figure 8). Through Egger’s test, bias was found to be non-significant (p = 0.257), as indicated by the funnel plot (Figure 9).
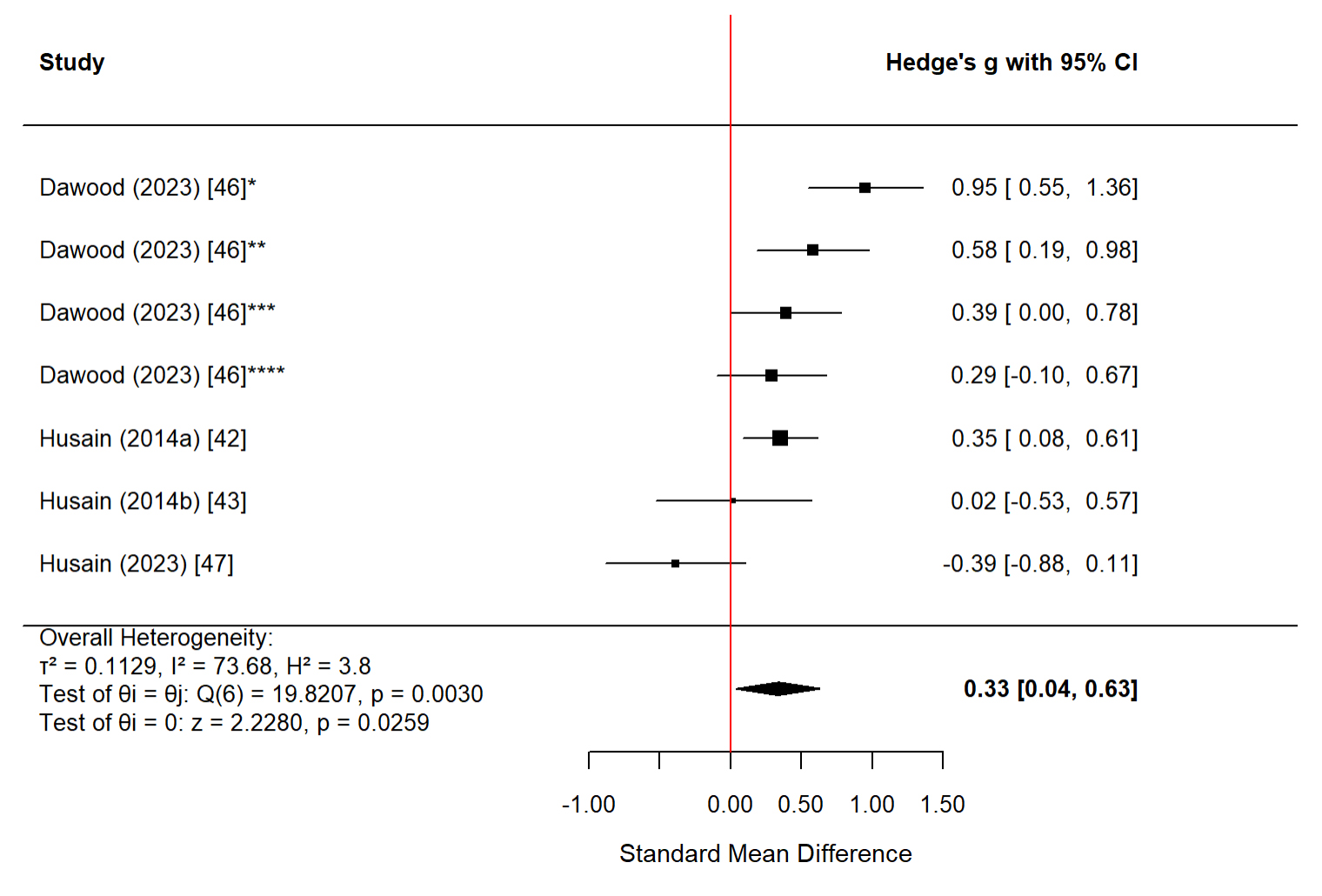 Figure 8.
Forest Plot of the Effect of CBT on Quality of Life in the South Asian Population Note. The following scales were used: WHOQOL-BREF (Physical Health, Psychological Health, Social Relationship, Environment) [46], Quality of Life Visual Analogue Scale (QOL-VAS) [42], and EuroQol 5-Dimension (EQ-5D) [43,47]. *WHOQOL-BREF Physical Health Domain. **WHOQOL-BREF Psychological Health Domain. ***WHOQOL-BREF Social Relationship Domain. ****WHOQOL-BREF Environment Domain. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
Figure 8.
Forest Plot of the Effect of CBT on Quality of Life in the South Asian Population Note. The following scales were used: WHOQOL-BREF (Physical Health, Psychological Health, Social Relationship, Environment) [46], Quality of Life Visual Analogue Scale (QOL-VAS) [42], and EuroQol 5-Dimension (EQ-5D) [43,47]. *WHOQOL-BREF Physical Health Domain. **WHOQOL-BREF Psychological Health Domain. ***WHOQOL-BREF Social Relationship Domain. ****WHOQOL-BREF Environment Domain. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
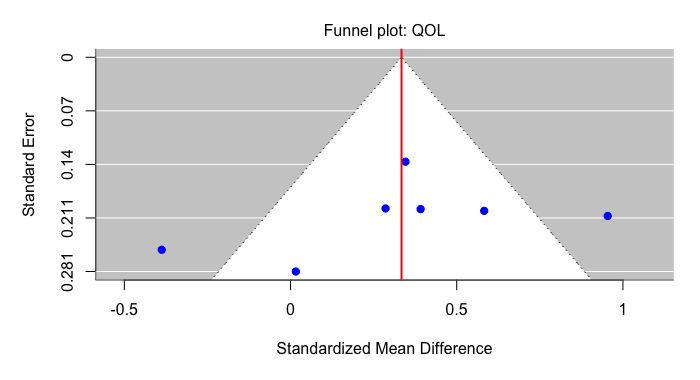 Figure 9.
Funnel Plot of the Effect of CBT on Quality of Life in the South Asian Population Using a Random-Effect Model Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
Figure 9.
Funnel Plot of the Effect of CBT on Quality of Life in the South Asian Population Using a Random-Effect Model Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
A total of four studies examined the effects of CBT on social support among South Asian populations. A total of 1803 individuals were included in these studies, with 911 participants in the treatment group and 892 participants in the control group. The mean age across studies was 27.74 years, with standard deviations ranging from 4.6 to 5.5. All participants included were South Asian. The studies included in this analysis were conducted in Pakistan (n = 3) and the United Kingdom (n = 1).
Figure 10 presents a forest plot of social support outcomes (n = 4). CBT was associated with a small increase in social support among South Asian participants; however, the pooled effect did not reach statistical significance (g = 0.20, 95% CI [−0.05,0.45], p = 0.12). Considerable heterogeneity was observed across studies (Q(3) = 14.74, p = 0.002, I2 = 78.68%), indicating substantial variability in effects across study contexts and designs. Funnel plot inspection and Egger’s regression test did not indicate significant publication bias (Figure 11). Trim-and-fill analysis suggested two potentially missing studies on the right side of the funnel; after adjustment, the pooled effect size increased and became statistically significant (g = 0.38, 95% CI [0.07,0.70], p = 0.016). Given the small number of included studies, these adjusted estimates should be interpreted cautiously.
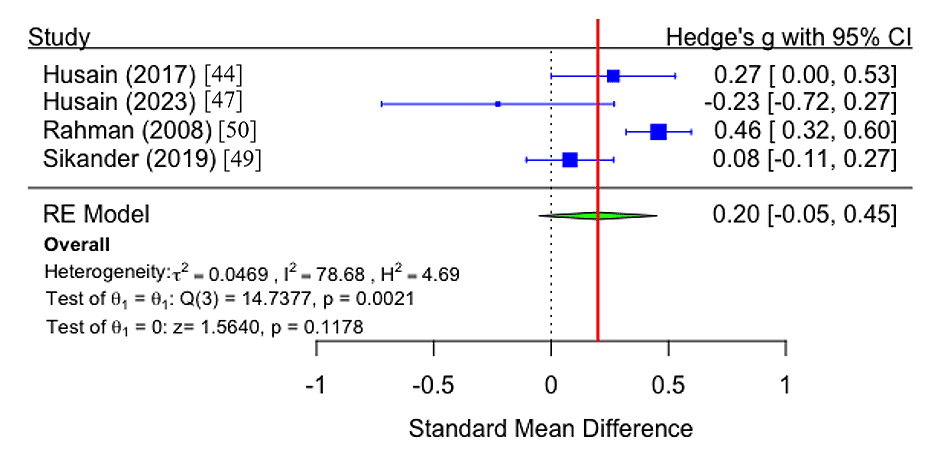 Figure 10.
Forest Plot of the Effect of CBT on Social Support in the South Asian Population Note. The following scales were used: Multidimensional Scale of Perceived Social Support (MSPSS) [44,47,49,50]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
Figure 10.
Forest Plot of the Effect of CBT on Social Support in the South Asian Population Note. The following scales were used: Multidimensional Scale of Perceived Social Support (MSPSS) [44,47,49,50]. The black squares represent the individual study effect sizes, with the size of each square proportional to the study weight in the meta-analysis; the black diamond represents the overall pooled effect size from the random-effects model, with the width of the diamond indicating the 95% confidence interval.
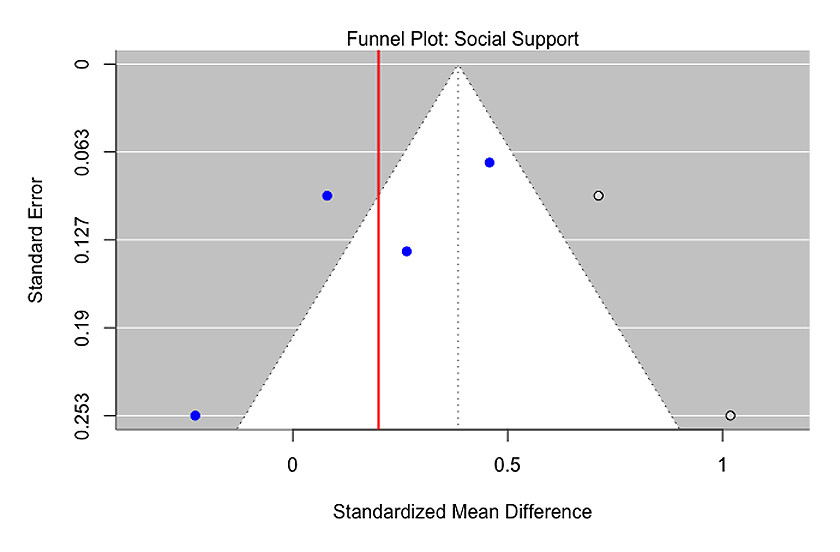 Figure 11.
Adjusted Funnel Plot of the Effect of CBT on Social Support in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
Figure 11.
Adjusted Funnel Plot of the Effect of CBT on Social Support in the South Asian Population Using a Random-Effect Model. Note. The blue circles represent the original observed studies included in the meta-analysis; the white circles represent the imputed study added by the trim-and-fill method to correct for potential publication bias. The vertical red line indicates the pooled effect size from the random-effects model.
There was only one study that measured PTSD, and thus, this variable was removed from analysis; other studies are cited descriptively. However, this study reports implications for significant PTSD symptom reduction [39]. Latif et al. examined the role of a culturally adapted, trauma-focused and CBT-based guided self-help intervention for female victims of domestic violence in Pakistan. Their RCT of 50 participants unveiled a significant reduction in PTSD symptomatology for the intervention group, suggesting the importance of examining the associations among CBT for South Asians and PTSD variable outcomes. CBT-derived interventions have been found to help reduce PTSD outcomes among Pakistani spinal cord injury patients [51], female refugees in Malaysia through culturally adapted group CBT interventions [52], and among male Afghan refugees undergoing culturally-adapted CBT interventions [53]. CBT interventions have also aided with PTSD symptom reduction for other populations, including those of Latino descent experiencing treatment-resistant PTSD [54].
Risk of BiasStudy quality was assessed using the Cochrane Risk of Bias tool (Table 2). Randomization was appropriately conducted in most studies, with low risk in 14 of 16 trials (87.50%) and unclear risk in 2 trials (12.50%). Allocation concealment was adequately implemented in 11 out of 16 trials (68.75%), with 1 trial (6.25%) rated as high risk and 4 trials (25.00%) rated as unclear. Blinding of participants and personnel was a key methodological limitation, with low risk in 7 of 16 studies (43.75%), unclear risk in 5 (31.25%), and high risk in 4 (25.00%). Blinding of outcome assessors was considered low risk in 8 of 16 trials (50.00%), unclear in 7 (43.75%), and high risk in 1 (6.25%). Incomplete outcome data or attrition bias, reflecting the completeness of outcome data, was considered low risk in many studies: 15 out of 16 trials (93.75%) were rated low risk, and 1 (6.25%) was rated high risk. Selective outcome reporting was consistently low risk, with all 16 trials (100%) judged to be low risk in this domain. Other potential sources of bias, such as recruitment methods, sample variability, and response bias, were rated as low risk in 12 of 16 studies (75.00%), unclear in 2 (12.50%), and high risk in 2 (12.50%). Overall, these findings indicate a mixed risk of bias across methodological domains, with concerns about blinding procedures, while most studies demonstrated adequate randomization, outcome reporting, and handling of missing data across aspects of study design and conduct within the included randomized controlled trials.
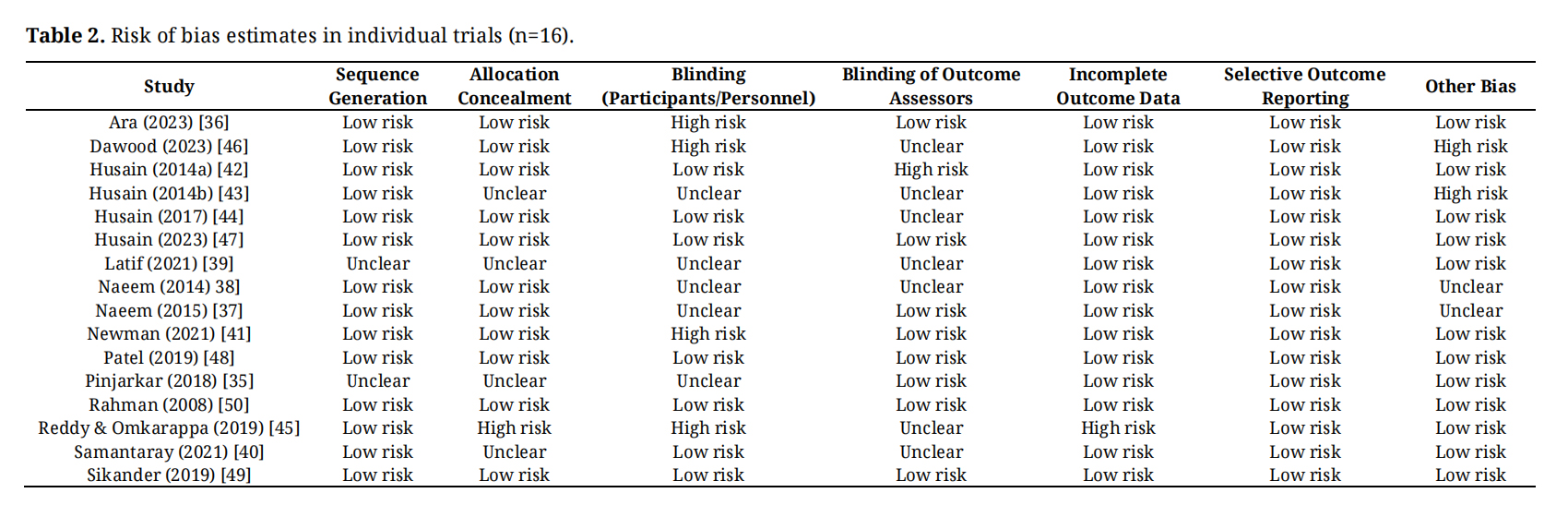 Table 2. Risk of bias estimates in individual trials (n=16).
Table 2. Risk of bias estimates in individual trials (n=16).
To our knowledge, this article is the first meta-analysis focusing exclusively on randomized controlled trials of cognitive behavioural therapy among South Asian adults, including both individuals residing in South Asia and those in diaspora settings. Although previous meta-analyses have examined culturally adapted psychosocial interventions in non-Western contexts [18,19], these reviews did not focus specifically on CBT for South Asian populations, nor did they restrict inclusion to RCTs or examine both origin-country and diaspora settings. Given the high prevalence of depression and anxiety globally and within South Asian populations, and the fact that South Asia represents approximately one-quarter of the world’s population, it is important to evaluate the effectiveness of accessible and scalable treatments such as CBT in this context.
The findings of this meta-analysis suggest that CBT interventions may contribute to improvements across several mental health outcomes in South Asian populations, including reductions in depression and anxiety symptoms. Consistent with previous work [18], CBT was associated with symptom reduction in both conditions; however, heterogeneity exceeded 90% for depression, anxiety, and disability, indicating substantial variability in treatment effects across study contexts, intervention formats, and delivery methods. Improvements were also observed in quality of life and disability outcomes, while the pooled effect for social support did not reach statistical significance. Accordingly, pooled estimates should be understood as average effects across heterogeneous trials rather than evidence of uniform efficacy. In particular, the pooled depression estimate may have been influenced by a small number of studies with exceptionally large effects, and should therefore be interpreted with caution. Confidence in pooled estimates differed by outcome, with depression analyses comprising a larger number of studies and showing greater heterogeneity and evidence of publication bias, whereas anxiety analyses were based on fewer trials and demonstrated borderline or non-significant small-study effects.
Consistent with previous work, CBT interventions, including several that incorporated cultural adaptations, were found to reduce anxiety and depression symptomatology among South Asian populations. This includes male Afghan refugees who experienced improvements through culturally adapted CBT [53], female refugees experiencing lower levels of emotional distress through group interventions [52], female victims of domestic violence in Pakistan showing improvement in depression and anxiety symptoms [55], and reduction in perinatal depression [56]. Moreover, CBT paired with pharmacotherapy helped with major depressive disorder among individuals in Pakistan [57], while being adapted as a digital intervention to reduce anxiety symptoms among college students in India [58], and in reducing depression and anxiety symptoms among patients experiencing distress in Pakistan [59].
The strong effects observed in South Asian populations may reflect cultural congruence between CBT’s principles and certain South Asian values, such as self-reflection, collective responsibility, and the emphasis on balancing thought and emotion. In contexts where mental health stigma remains prevalent, CBT’s structured, goal-oriented, and problem-solving approach may offer a culturally acceptable framework for addressing emotional distress. As noted in the literature, “cultural adaptation of CBT focuses on three main areas: awareness of culture and related issues, assessment and adjustment in therapy techniques” [60]. These results affirm CBT’s flexibility and suggest that culturally informed modifications, such as integration of family dynamics, spiritual beliefs, or culturally specific idioms of distress, may further enhance treatment outcomes.
This evidence also challenges the assumption that Western psychotherapeutic models necessarily lack cross-cultural validity. Rather than requiring fundamentally different frameworks, the present results suggest that CBT’s core mechanisms of cognitive restructuring and behavioural activation are relevant psychological processes that can be meaningfully applied across cultures. Supporting this, a knowledge synthesis found that culturally adapted CBT “demonstrated significant effectiveness in reducing symptoms of depression, anxiety, PTSD, and psychosis among various cultural groups” [61]. From a clinical and policy perspective, these findings underscore the potential for scaling up CBT-based interventions within South Asian and other non-Western populations as part of global mental health strategies.
Eight studies employed culturally adapted CBT protocols and reported consistent moderate to very large effect sizes across diverse settings (d = 0.89–4.75), while three studies using standard CBT without explicit adaptation showed large effects (d = 0.86–1.22), all for anxiety disorders. Five studies implementing specific CBT elements or components showed more heterogeneous outcomes (SMD = −0.13 to −0.30), with behavioural activation showing promise when combined with problem-solving or family involvement. The pattern suggests that complete, coherent protocols, whether culturally adapted or standard, may be more effective than partial implementations, particularly for mood disorders.
Pakistan (n = 9) predominantly used culturally adapted CBT (67%) with a strategic focus on perinatal depression and peer- or lay-delivered formats. India (n = 5) showed the inverse pattern: 60% used standard CBT without explicit adaptation, concentrated on anxiety disorders in urban educational settings. This geographic divergence may reflect different healthcare contexts rather than clinical evidence; Pakistan’s limited specialist workforce necessitated cultural adaptation and lay delivery, while India’s urban research centres had access to trained clinicians. The single UK diaspora study [47] underscores an evidence gap regarding whether South Asian cultural adaptations translate to immigrant populations.
Individual delivery (n = 5) achieved the largest effect sizes (d = 0.93–4.75) but requires the most resources. Group delivery (n = 5) showed large effects for anxiety and depression when attendance was adequate but lower engagement in diaspora settings. Self-help with minimal guidance (n = 4) achieved moderate to large effects (d = 0.40–1.9) and superior scalability, while peer-delivered interventions (n = 2) achieved moderate effects at lowest cost. The evidence does not support a single superior format; instead, effectiveness appears contingent on population engagement and local resource capacity.
Perinatal depression (n = 4) was disproportionately researched relative to its burden and consistently benefited from culturally adapted CBT. Anxiety disorders (n = 3) showed particularly large effect sizes and appeared less dependent on cultural adaptation, possibly reflecting more universal symptom presentations. Complex presentations including trauma, self-harm, and psychosis (n = 3) showed promise with specialised adaptations but remain underresearched.
The included studies were predominantly conducted in South Asia (n = 15) with only one study in a diaspora setting (Husain et al. (2023) [47]: British South Asian women with postnatal depression in the United Kingdom). Studies in Pakistan, India, and Bangladesh were delivered within the cultural contexts in which participants lived, embedded in family systems, community structures, and healthcare settings shaped by local norms. Cultural adaptation in these settings focused on incorporating local values, family involvement, and adaptation to limited healthcare resources. Effect sizes were generally large across diverse delivery formats and populations.
The single UK study enrolled British South Asian women receiving care through the National Health Service. Notably, this study found no significant intent-to-treat difference between culturally adapted group CBT and treatment as usual on the primary outcome (HDRS at 3 or 6 months; p > 0.05). The observed effect size was substantially smaller than anticipated (d = 0.10–0.16 vs. anticipated d = 0.9), suggesting underpowering. Despite culturally sensitive adaptations, including ethnically matched facilitators and delivery in participants’ preferred language, engagement was lower and outcomes were modest compared to the Pakistani perinatal studies.
Several factors may explain differential outcomes between origin-country and diaspora settings: acculturation may reduce the salience of adaptations emphasising family involvement and religious coping; universal healthcare in the UK may leave less room for improvement relative to resource-limited South Asian settings; and competing demands on diaspora women’s time may limit attendance and completion. This limited evidence suggests that cultural adaptation developed for South Asian contexts does not automatically translate to diaspora populations and that effective adaptation may be context-specific rather than population-specific.
These findings carry several practical implications. For clinicians, the evidence suggests that cultural adaptation enhances outcomes for mood disorders, though anxiety disorders appear responsive to standard protocols. Lay counsellor delivery is effective when protocols are clear and supervised, and family involvement consistently strengthens outcomes. Protocol fidelity appears to matter more than therapist credentials, supporting task-shifting approaches in resource-limited settings.
For patients, the findings indicate that CBT is associated with moderate to large reductions in depression, anxiety, and trauma symptoms, with outcomes typically peaking at 3 to 6 months. Self-help with minimal guidance achieves outcomes comparable to intensive therapy, and non-specialist providers deliver care as effectively as specialists in the studies reviewed.
For healthcare systems, task-shifting to lay counsellors represents a cost-effective and evidence-based strategy. Brief 6 to 8 session formats appear as effective as longer treatments. Multiple delivery formats achieve broadly similar outcomes, suggesting that systems should diversify according to local capacity. Systematic attention to accessibility barriers, including transportation, childcare, and stigma, and integration with existing structures such as primary care and maternal health services, are likely to enhance reach and sustainability.
Overall, these findings suggest that standard and culturally adapted CBT interventions may prove useful for several mental health outcomes among South Asian adults. However, the variability in effectiveness highlights the need to adapt these interventions further and integrate cultural considerations in ways that enhance applicability, particularly for those experiencing depression and anxiety.
LimitationsThe small number of included trials (k = 16) reflects the novel focus of this review. The extremely high heterogeneity observed across most pooled analyses (I2 > 90% for depression, anxiety, and disability) further limits the interpretability of summary effect sizes and suggests that treatment effectiveness may be highly context-dependent. Evidence of publication bias was also detected through funnel plot inspection and Egger’s test, indicating that the pooled estimates may overstate the true effect. Because some studies contributed multiple effect sizes for the same outcome, the pooled estimates may reflect statistical dependence within studies. As robust variance estimation or multilevel meta-analysis was not applied, standard errors may have been underestimated and precision overstated.
Two studies reported exceptionally large effect sizes with wide confidence intervals: Ara et al. (2023) [36]; g = −4.90) and Latif et al. (2021) [39]; g = −3.44). These studies may exert disproportionate influence on the pooled depression estimate. A formal leave-one-out sensitivity analysis was not conducted because the review was pre-registered with a specified analytic protocol (PROSPERO: CRD42025631254) that did not include post hoc influence diagnostics. We acknowledge, however, that the absence of such analyses limits our ability to quantify the extent to which individual high-leverage studies may have affected the pooled estimate. The trim-and-fill adjusted estimate (g = −1.49, 95% CI [−2.28,−0.71]) provides some reassurance that the pooled effect remained significant after accounting for small-study effects, but the magnitude of the pooled depression effect should nevertheless be interpreted cautiously.
The interval between the initial June 2020 search and the February 2024 update may have resulted in delayed identification of eligible studies. However, the 2024 update did identify additional studies published during this period, suggesting that recent evidence was successfully captured.
The inclusion of conceptually distinct CBT-based interventions, including acceptance and commitment therapy, dialectical behaviour therapy, mindfulness-based interventions, and behavioural activation, alongside standard and culturally adapted CBT, represents a key source of heterogeneity. Pooling these intervention types may obscure meaningful differences in effectiveness. Subgroup analyses by intervention type were considered but were not feasible due to the limited number of studies within each category.
A substantial proportion of included trials were conducted in Pakistan (n = 9), with all studies contributing to the disability analysis originating from this context. Differences in healthcare systems, cultural norms, and service accessibility across South Asian countries may influence CBT effectiveness, limiting the generalisability of findings to other populations, including those in India, Bangladesh, Sri Lanka, and diaspora settings.
Although approximately 11 of the 16 studies reported follow-up assessments beyond the post-intervention time point, the present analysis focused on post-intervention effects to ensure consistency, given variability in follow-up timing and reporting methods. As a result, the findings primarily reflect short-term treatment outcomes, and conclusions regarding the long-term durability of CBT effects cannot be drawn.
The included studies varied in how “South Asian populations” were defined, and patient-level data on potential moderators such as age, sex, and socioeconomic status were inconsistently reported. This limited the scope for moderator analysis and precludes conclusions about which subgroups may benefit most from specific interventions.
Future DirectionsFirst, future meta-analyses should employ more rigorous statistical methods, including leave-one-out sensitivity analyses to assess the influence of outlier studies, and robust variance estimation or multilevel modelling to account for within-study dependency when multiple effect sizes are extracted from individual trials. More frequent or continuous search updates would also reduce the risk of missing eligible studies between review cycles.
Second, head-to-head comparisons of different CBT modalities, including standard CBT, culturally adapted CBT, behavioural activation, and mindfulness-based approaches, are needed to determine whether certain subtypes are more effective or culturally appropriate for South Asian populations. Dismantling studies that isolate specific adaptation components, such as family involvement, religious integration, or language modification, would clarify which elements drive treatment effects.
Third, research should expand beyond Pakistan to include more geographically diverse samples from India, Bangladesh, Sri Lanka, Nepal, and other South Asian countries. Equally important is the study of diaspora populations in the United Kingdom, Canada, the United States, and Australia, where acculturation, healthcare context, and social roles may require distinct intervention modifications. Participant inclusion criteria should also be refined to specify factors such as degree of South Asian ancestry, country of residence, and duration of residence, which may influence treatment response.
Further studies should compare CBT with other psychological and pharmacological interventions to determine the most effective approaches for treating depression and anxiety within South Asian populations. Expanding research to include additional psychosocial outcomes beyond depression and anxiety, such as quality of life and social support, will provide a more comprehensive understanding of intervention impact. Although the present review identified preliminary evidence for CBT’s effectiveness in reducing PTSD symptoms, this outcome was not included in quantitative analyses due to the limited number of studies. Prior research has demonstrated that trauma-focused CBT can reduce PTSD symptoms among specific South Asian populations [51], and previous studies suggest that CBT may be effective in reducing OCD symptoms among these populations [53,62–64,], highlighting the need for further investigation in both areas.
Finally, incorporating qualitative methodologies, including participant and therapist perspectives on intervention acceptability and engagement barriers, would complement quantitative findings and inform the development of more culturally responsive treatments. Dose-response studies examining optimal session length, treatment duration, and follow-up intervals are also needed, given the variability in intervention formats observed in the current review. Consistent reporting and synthesis of follow-up outcomes in future trials will be essential for understanding the sustainability of treatment effects.
Ethical review and approval were waived for this study as it is a systematic review and meta-analysis based solely on previously published studies. No individual participant data were collected or accessed, and no human subjects were directly involved in the research.
Patient consent was waived because this study is a systematic review and meta-analysis of previously published studies. No individual participant data were collected, and informed consent was therefore not required.
Trial Registration: This study is a systematic review and meta-analysis, not a clinical trial.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guideline was followed.
The following supplementary materials are available online, Flie S1: Search Strategy, Flie S1: Data Extraction Form.
The datasets generated and analyzed during the current study are publicly available in the Mendeley Data repository: https://doi.org/10.17632/ccfnt82fpt.1. All data are derived from published sources and contain no individual-level information.
VI and FN conceptualized and designed the study. VI, NA, MAK, SK, HA, ZW, AAC, RR, and SK contributed to data curation, investigation, and methodology. VI, NA, MAK, SK, and MA conducted the formal analysis and validation. VI and NA led the project administration and visualization. FN and MAK provided supervision and methodological oversight. VI, SK, NA, MAK, HA, ZW, AAC, and RR drafted the manuscript. VI, NA, FN, AAC, SK, and FN critically reviewed and edited the manuscript. All authors contributed to the interpretation of the data. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
The authors declare that there is no conflict of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The funding sources had no role in study design; data collection, analysis, or interpretation; manuscript preparation; or the decision to submit the work for publication.
The authors thank Rena Besa, Centre for Addiction and Mental Health, for assistance in developing and executing the search strategy in accordance with PRESS guidelines.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
Ip V, Kyte S, Arulventh N, Khan MA, Abbasian H, Wakif Z, et al. Cognitive Behavioural Therapy for South Asian Adults with Depression and Anxiety: A Systematic Review and Meta-Analysis. J Psychiatry Brain Sci. 2026;11(3):e260010.https://doi.org/10.20900/ipbs.20260010.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




