Location: Home >> Detail
Adv Geriatr Med Res. 2025;7(4):e250022. https://doi.org/10.20900/agmr20250022
 ,
Hélène Corriveau 2,3 ,
Julie Lapierre 1 ,
Geneviève Ricard 1 ,
Catherine Pagé 2 ,
Émilie Breton 1,2,*
,
Hélène Corriveau 2,3 ,
Julie Lapierre 1 ,
Geneviève Ricard 1 ,
Catherine Pagé 2 ,
Émilie Breton 1,2,*
1 Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie—Centre Hospitalier Universitaire de Sherbrooke (CIUSSS de l’Estrie—CHUS), 375 Rue Argyll, Sherbrooke, QC J1J 3H5, Canada
2 Research Centre on Aging, Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie—Centre Hospitalier Universitaire de Sherbrooke (CIUSSS de l’Estrie—CHUS), 1036 Belvédère South, Sherbrooke, QC J1H 4C4, Canada
3 School of Rehabilitation, Faculty of Medicine and Health Sciences, University of Sherbrooke, 3001 12e Avenue N, Sherbrooke, QC J1H 5H3, Canada
* Correspondence: Émilie Breton
Background: Tinetti demonstrated that falls among community-dwelling older adults can be prevented through a stepwise, individualized approach. However, in Canada, many current fall prevention clinics implement universal rather than customized interventions. This study evaluated the effectiveness of this original clinic approach on fall risk.
Methods: This was a pre-post single-group longitudinal study. At baseline, professionals, including nurses, physiotherapists, and geriatricians, conducted discipline-specific assessments. The team identified specific fall risk factors and proposed personalized, evidence-based interventions. A nurse conducted a structured follow-up to collect data on falls and the patient’s condition over six months, and a physiotherapist performed a final mobility assessment.
Results: Fifty-nine older patients referred to the Fall Prevention Clinic completed the study. The fall rate at six months dropped to 36% from 91% in the previous year (p < 0.001), suggesting two-thirds stopped falling. The most common risk factor was deconditioning (46%). No significant differences in risk factors or interventions were found between participants who fell and those who did not after the intervention, except referrals to community occupational therapy, which were more common among those who fell (p = 0.038). The key intervention, Exercise, was prescribed to 85% of the participants. Mobility assessments revealed no significant changes, except for an improvement in lower limb strength (p = 0.02).
Conclusions: Fall prevention requires precise identification of risk factors and prompt initiation of targeted interventions. Our model of an interprofessional Fall Prevention Clinic offers a comprehensive approach to identify key modifiable risks and reduce fall incidence in high-risk populations.
n, sample size; SD, standard deviation; TUG, Timed Up and Go; 5STS, Five Times Sit to Stand Test; walk test, 10-meter walk test
Falls remain the leading cause of injury-related hospitalization and death among Canadian seniors [1]. In 2018, in Canada, falls in older adults cost up to $5.6 billion in health services [1,2]. Even a minor fall can result in a decreased level of activity, leading to a loss of independence and isolation. In Canada, one-third of the older adults hospitalized after sustaining a fall are admitted to long-term care [3]. Falls are the result of additive health-related problems that are ignored or wrongly tolerated by the elderly person, their relatives and the healthcare system [4]. To mitigate an individual’s risk of falls, the most likely and the most severe risks of falls must be identified [5].
Tirrell et al., 2015, demonstrated that in an urban Level I trauma center teaching hospital Emergency Department, the current evaluation of older adult fallers is inconsistent with both general and ED-specific fall guidelines [6]. As a result, causative health problems remain unresolved, leading to further falls. For instance, most patients will find their polypharmacy unchanged after assessment in the emergency department [7,8]. Nonetheless, the Emergency Department may not be the most relevant or efficient environment for a thorough geriatric assessment, which requires time and sometimes specialized expertise, as is often available in most geriatric clinics.
Successful studies showed that the risks of falls can be reduced with direct interventions on vision, balance, gait problems, muscle weakness, joint diseases, disabling foot pain, psychotropic drugs, sedatives, anti-hypertensive medications, cardioinhibitory carotid sinus hypersensitivity, and environmental factors [9,10]. Most of the seniors who fall exhibit a complex combination of multiple fall risk factors, making single and universal interventions ineffective in reducing fall risk [11]. Tinetti et al. (1988) [12] recommended the use of a stepwise individualized approach to minimize the risk of falls: Establish defined fall risk factors, deal with individual medical and social considerations, and manage with tailored multifaceted interventions directly aimed at mitigating the identified risk factors. A 2018 Cochrane meta-analysis indicated that tailored, multifactorial interventions based on Tinetti’s recommendations could reduce fall rates more effectively than strategies targeting just one risk factor [13]. The World Falls Guidelines (WFG) Task Force stated in 2022 [14] that “Multidomain interventions encompass two or more components, individually targeted to the older adult based on findings from a multifactorial (or comprehensive) falls risk assessment. It is not a standardized set of interventions applied to everyone,” meaning that professionals should tailor their interventions to reduce the risk of falls to the individual’s specific risk factors identified by a comprehensive assessment.
Fall Prevention Clinics appear to reduce fall rates and enhance daily activities [8,15–19]. However, most RCTs on fall prevention clinics have focused on a single intervention—such as deprescribing—or a standard physical exercise program, or a small set of combined strategies. Davis et al. [4] demonstrated that implementing a multifactorial, geriatrician-led, evidence-based Falls Prevention Clinic for older adults with a history of falls is both feasible and well accepted. To our knowledge, aside from Davis’s team, no studies have addressed all risk factors simultaneously within a single setting, including deprescribing or appropriate prescribing, environmental modifications, assessment and prescription of the correct walking aid, and a fully tailored physical activity program. Furthermore, most prior studies excluded patients at much higher risk of falling, such as those with dementia, Parkinson’s disease, and a history of stroke.
Therefore, our team suggested a design for a Fall Prevention Clinic: a comprehensive, stepwise geriatric assessment and individualized interventions targeted at specific risk factors, as previously recommended by Tinetti [12]. This approach was implemented during a single visit to the Fall Prevention Clinic located within an external university-affiliated geriatric specialty clinic in Quebec, with subsequent follow-up monitoring. This is the first Fall Prevention Clinic of its kind in the Province of Québec, specifically including patients at very high risk of falling. In this study, the specific objectives were: (1) To assess the effectiveness of this original clinic approach on the risk of falls and mobility loss over 6 months, and (2) to identify who benefits the most from the intervention regarding fall risk reduction.
This was a pre-post single-group longitudinal study. We included all older patients consecutively referred to the Fall Prevention Clinic. The clinic is funded through public resources and is situated within a university hospital in Sherbrooke, Quebec, a community characterized by a balanced distribution of rural and urban populations. Referrals are made by primary care physicians and hospital specialists, with the majority originating from emergency physicians. Our operational model stipulates that patients experiencing or recovering from an acute medical condition follow an in-hospital pathway for assessment and geriatric rehabilitation, rather than being directed to external clinics. Therefore, most patients sent to the clinic are in stable condition.
Participants were initially assessed (T1) by the interprofessional team (nurses, physiotherapists, geriatricians) during a single appointment lasting approximately 2.5 h. All clinicians were trained to perform their discipline-specific assessments. A structured over-the-phone 6-month follow-up was then conducted to collect data on falls and on the patient’s condition. Finally, a second mobility assessment was performed at the end of the follow-up period (T2, at 6 months) by the physiotherapist.
On the day before the in-person visit, the nurse provided explanations to the patients about the project and confirmed their appointment at the Fall Prevention Clinic. Patients signed the consent form at their initial in-person visit if they were willing to take part in the project.
Multidisciplinary Fall Risk Assessment Fall Risk AssessmentBased on the literature, our research team created a fall questionnaire including crucial information about the history of falls in the past 12 months, different components of functional autonomy, and sociodemographic characteristics. A team of experts, including 4 geriatricians, 1 Ph.D. expert on falls in seniors, 1 clinically skilled nurse in geriatrics, and 1 physiotherapist, reviewed the questionnaire twice and adopted it consensually. The questionnaire was supported by an Android tablet application that allowed the information to be securely uploaded to our database. To avoid overburdening the patient during the in-person visit and to increase efficiency, the fall questionnaire was administered by a nurse over the phone, a few days before the visit and was made available to the other clinicians before the appointment.
During the first appointment (T1), clinical data were collected by the nurse, including postural blood pressure, cognitive testing (Folstein, clock drawing test) [20] and functional status. The geriatrician performed a focused medical assessment to identify medical conditions involved in the fall risk, with special attention to neurological and locomotor conditions and fall history. Afterwards, the team documented and prioritized the patient’s main issues leading to falls in a grid. The interdisciplinary team previously developed a grid, listing various conditions associated with falls: Neurological (superior central, middle central, peripheral), psychogenic (fear of falling), locomotor (spine, lower limbs), polypharmacy, cardiovascular (syncope, orthostatic hypotension, hypotension), metabolic, visual (decreased visual acuity), poor general condition, deconditioning (loss of endurance, cardiovascular capacity, and/or strength caused by a sedentary lifestyle or chronic condition), psychosocial issues, podiatric problem affecting locomotion, lack of social support, and high risk behaviors. A classification suggested by Nutt [21] inspired the division of the Gait Syndromes that can result in falls in older patients. From the identified conditions that could increase the patient’s risk of falling, the team prioritized the 3 most severe, life-threatening, or reversible. All other identified significant medical, environmental, and psychosocial issues were addressed.
The physiotherapist evaluated mobility, balance [22] and grip strength [23]. He collected those dependent variables at inclusion (T1) and 6 months post-intervention (T2): Functional lower limb strength and gait parameters through the 5STS [24], the TUG [25], and walk test [26]. The physiotherapist used the Mobility lab® throughout his assessments, a body-worn sensor system easily used by clinicians [27,28].
Interdisciplinary Meeting and Targeted InterventionsAfter the single-session multidisciplinary assessment, all participating professionals reached a consensus regarding the identified fall risk factors. They developed a personalized, evidence-based intervention plan to mitigate the risk of future falls. The tailored plans may include stopping certain medications deemed problematic for a specific patient, implementing physical activities suitable to the patient’s level of independence and frailty within the scope of available programs in Quebec’s public and community organizations, prescribing walking aids, if necessary, as well as referrals to home occupational therapy, social services, or nutrition experts. The geriatrician recommended further investigations and scheduled follow-up appointments as required. Deprescription was encouraged if the Geriatrician identified a medication directly linked to the patient’s fall risk and that appeared on the revised 2019 AGS Beers criteria [29]. Numerous public and community physical activity programs are available in Québec, targeting a range of older adults, from those who are very frail to those who are very fit. The geriatrician and physiotherapist selected the appropriate program for each patient, who then acknowledged it. Home safety assessments were facilitated through referrals to available community occupational therapy.
Falls Follow-UpsThe dependent variables included the number of participants who experienced at least one fall after the intervention. A fall was defined as “an event in which the resident [patient] unintentionally came to rest on the ground or floor, regardless of whether an injury was sustained” [30]. Fall ascertainment was conducted using a calendar provided to each patient. Additionally, the nurse performed three 10-min follow-up calls to gather information about falls recorded on the calendar and to discuss these incidents with the patient and their caregiver at 1, 3, and 6 months after the initial assessment. During these calls, the nurse also addressed any questions the participants had regarding their conditions and interventions. This strategy was effective in capturing most falls, as demonstrated in a previous study [31].
AnalysisParticipants’ characteristics, functional and physical abilities, were described at pre-intervention (T1) using means and standard deviations (continuous variables) or frequency and percentages (categorical variables).
The McNemar test was used to determine if there was a difference between the number of patients who sustained at least one fall pre-intervention (within a previous period of 12 months) and post-intervention (6-months period and exclusively from 3–6 months).
The Exact Fisher test was used to identify differences in the identified fall risk factors between patients who fell and those who did not after the intervention (between 3–6 months post-intervention).
A Wilcoxon signed rank test was used to analyze whether the intervention influenced mobility parameters between pre- and 6-month post intervention (STS, TUG, and walk test (gait speed)). Data were analyzed using IBM SPSS Statistics version 24.0 (IBM Corp., Armonk, NY, USA).
We recruited 60 participants who consecutively visited the Fall Prevention Clinic, from September 2018 to March 2019. Only 1 participant was excluded because he had already been evaluated in a similar program.
Of the remaining 59 participants who completed the entire 6-month follow-up: Two (2) died, and 13 dropped out for various reasons (cognitive deficits that became too severe, admission to a nursing home, or no interest in participating anymore). A CONSORT Flowchart figure is provided in Appendix A. At baseline, there was no significant difference in sociodemographic and clinical data between the patients who fell and those who did not after the intervention (Table 1).
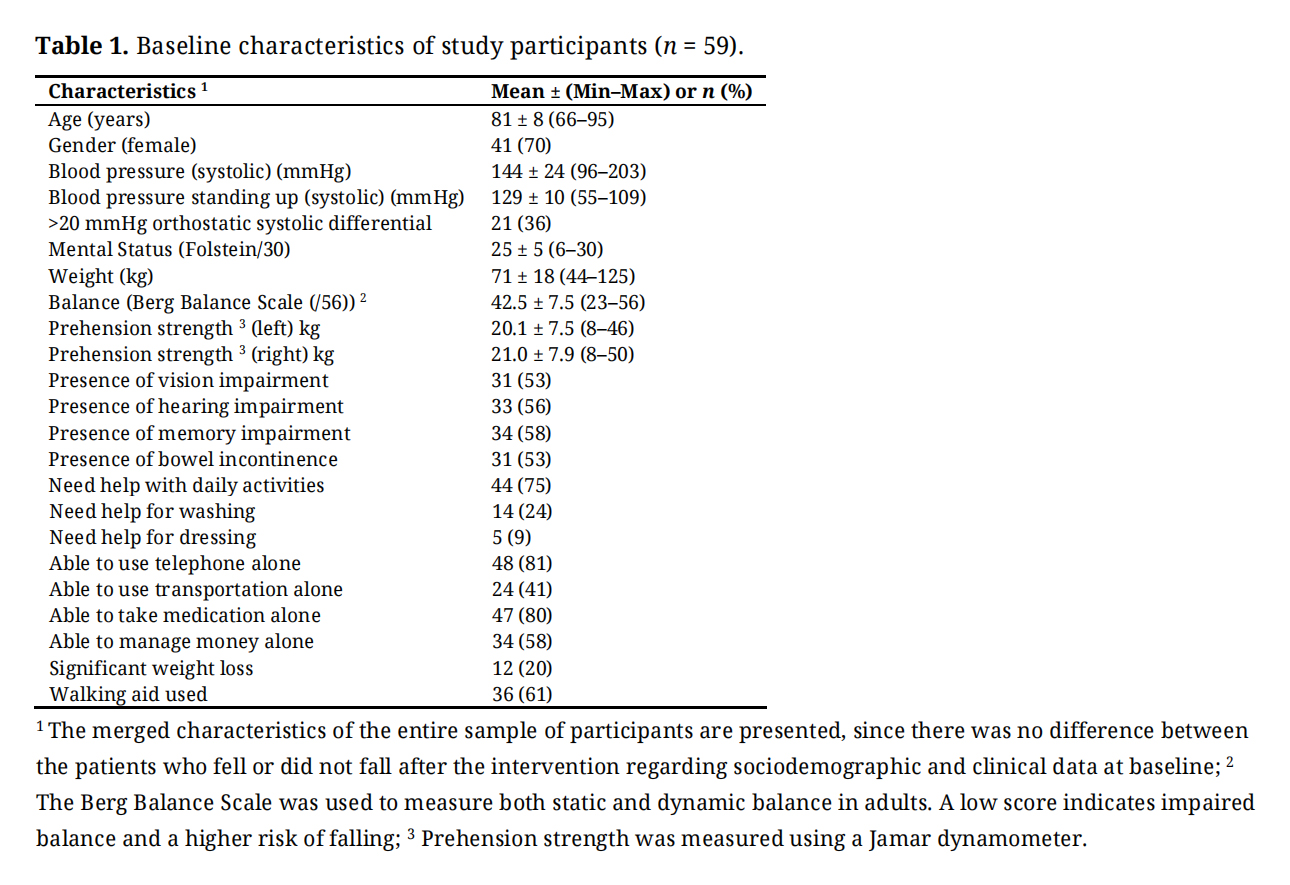 Table 1. Baseline characteristics of study participants (n = 59).
Table 1. Baseline characteristics of study participants (n = 59).
Ninety-one percent (91%) of participants had sustained a fall in the 12 months before enrolment. Thirty-six percent (36%) (n = 16/44, p < 0.001) of the participants sustained at least 1 fall during the 6-month period following the intervention. If the interval covered was limited to the 3–6 months post-intervention period, the proportion of participants experiencing at least one fall declined to 20%. (n = 9/44, p < 0.001).
Fall Risk Factors and InterventionAmong all the identified conditions that could increase a patient’s risk of falling, the team prioritized the three conditions that are most severe, life-threatening, or reversible for each individual patient, then ranked them accordingly. The most frequent medical fall risk factor was deconditioning (21%), followed by both peripheral neurological disorder (14%), and superior central neurological disorder (14%). When the three risk factors most likely to provoke falls in a given individual were combined, deconditioning remained the most frequent risk factor (46%). The prevalence of Superior Central neurological condition (36%) and Middle Central neurological condition (stroke, Parkinson’s Disease, etc.) (21%) was quite high in our study cohort. There was no statistical difference between the patients who fell and those who did not after the intervention in their principal fall risk factor, but some when the three ordered risk factors were pooled. There was a greater frequency of the risk factor “psychogenic” (fear of falling) in the patients who did not fall after the intervention (p = 0.047). The frequency of the risk factor “middle central neurological” (stroke, Parkinson’s Disease...) was statistically greater (p = 0.042) in the patients who fell after the intervention than in the patients who did not (Table 2). Among the patients who exhibited “cognitive disorders” as their primary risk factor, 11% did not fall after intervention and 33% did fall, but without statistical difference.
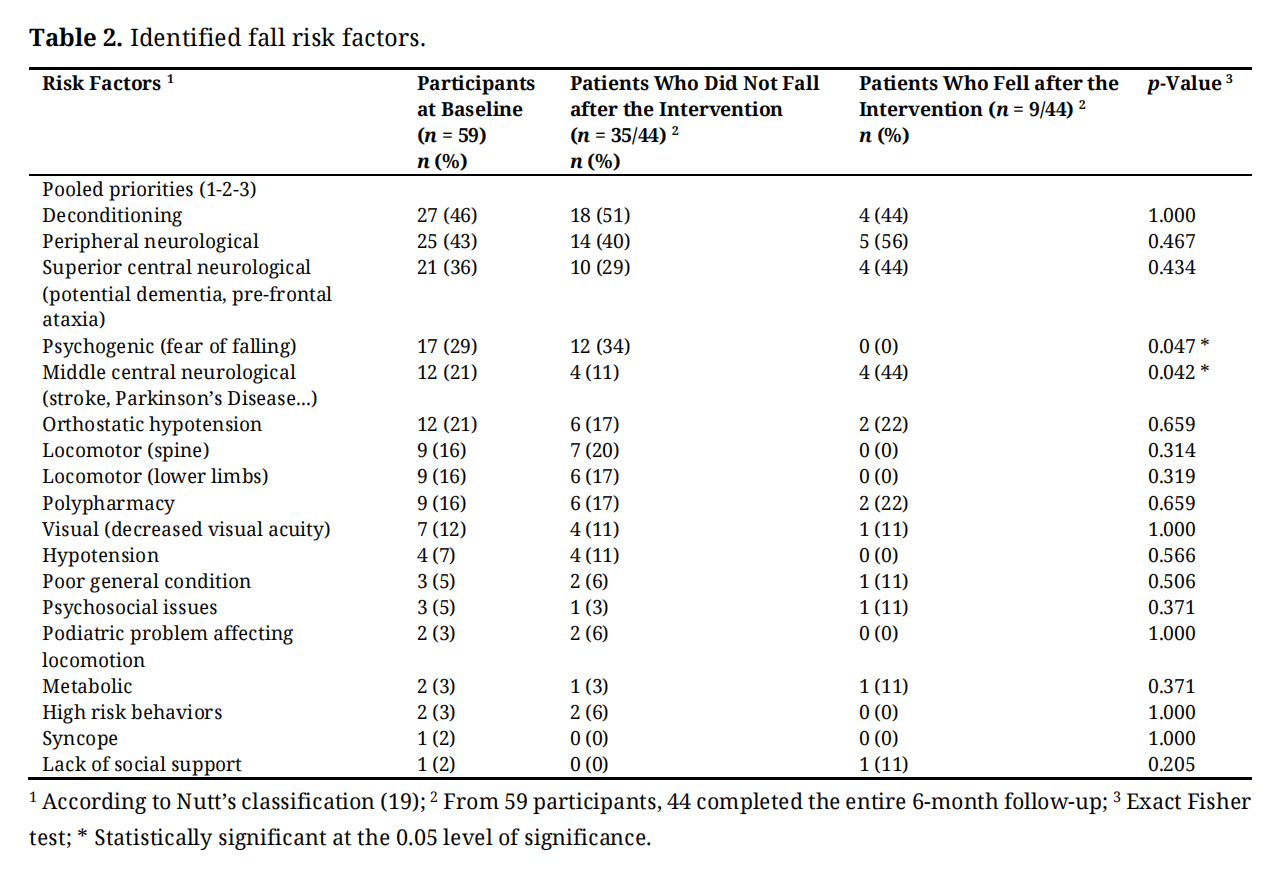 Table 2. Identified fall risk factors.
Table 2. Identified fall risk factors.
Concerning the type of interventions suggested, there was no statistical difference between the patients who fell and did not fall after the intervention, other than the patients who fell were slightly more often referred to community occupational therapy (p = 0.038). The main intervention prescribed for the participants who did not fall after the intervention was physiotherapy at home (54%). In this study, part of the intervention involved identifying the most appropriate type of physical activity program for each patient. We offered guidance and support to help patients engage with the appropriate public or community programs, tailored to their walking capabilities, balance levels, and degree of frailty. Exercise in any of these programs was prescribed for 85% of the participants. The patients who fell after the intervention were thought to require a medical follow-up in 67% of the cases, compared to 34% in patients who did not fall after the intervention. Most geriatricians scheduled a follow-up when the patient required further investigations or was deemed at higher risk of falls (Table 3)
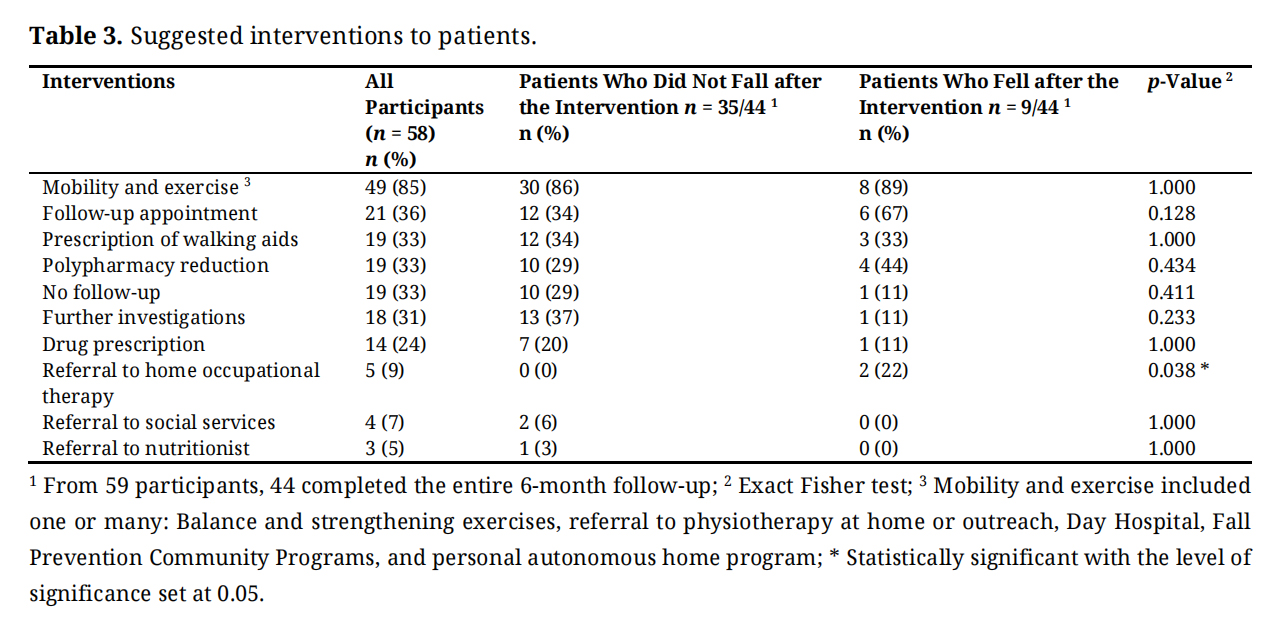 Table 3. Suggested interventions to patients.
Table 3. Suggested interventions to patients.
Although no statistically significant difference was observed in pre- and post-intervention scores for the TUG and walk test, there was a significant improvement in mean lower limb strength as measured by the 5STS (20.8 s ± 7.7 s vs. 17.1 s ± 6.6 s; p = 0.02) (Table 4). Clinically, this change corresponds to a mean reduction of 3.6 s on the 5STS. The minimal clinically important difference for the 5STS is approximately 3 s, based on the study by Agustín et al. [32].
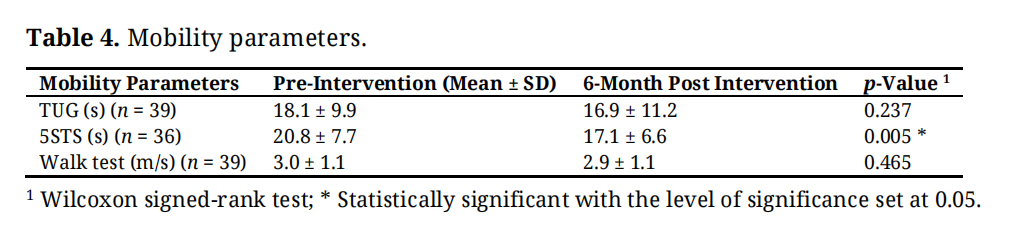 Table 4. Mobility parameters.
Table 4. Mobility parameters.
In this pilot study, we evaluated the impact of an innovative Fall Prevention Clinic model. Our clinic included patients with various medical conditions that lead to falls, which were excluded from most previous Fall Prevention clinic studies, such as stroke, Parkinson’s disease, and dementia. With the expertise of a team comprising a geriatrician, a physiotherapist, and a specialized nurse, we specifically addressed patients’ personal health and environmental factors contributing to falls, including medical management, environmental modifications, and tailored physical activities. Additionally, in the Province of Quebec, this is the first clinic of its kind: most patients who fall and are evaluated by subspecialists in internal medicine, emergency physicians, family doctors, pharmacists, physiotherapists, or occupational therapists usually only get assessed within their own specialty without reconciling all fall risk factors or coordinating specific interventions, especially regarding medication. Our geriatrician-led clinic addresses a much broader range of fall risk factors all at once. Overall, we are pleased that our design of a Fall Prevention Clinic showed a trend towards reducing the risk of falls in our population, even though they were often very frail and suffering from neurological conditions that kept those patients from participating in previous fall prevention clinic studies. Indeed, despite a potential recall bias, among the 91% of participants who had at least one fall during the year preceding the intervention, only 36% sustained a fall during the 0–6 months post-intervention interval, and 20% during the 3–6 months post-intervention interval. We decided to consider analyzing the 3–6 months interval, considering delays (3 months) before initiation of physical and exercise therapy, and interventions on environmental and personal factors (e.g., effects of slow medication changes).
A study by Lord et al. (2005) [17] demonstrated that participating in an individualized fall prevention program, which includes an exercise component over 12 months, can reduce the relative risk of falls by approximately 20%. This average reduction in fall risk aligns with the findings of this study.
The 5STS correlates with falls: Nevitt et al. (reported in Bohannon et al. [24]) indicated that taking more than two seconds to complete one sit-to-stand increases fall risk by 2.4. Our intervention improved 5STS by 3.6 s, aligning with increased strength and physical capacity, likely mainly due to the physical activity component of the overall approach. Also, the intensity of strengthening exercises has the potential to better prevent falls, as improvements in strength and physical capacity appear to be key factors in the trend of reducing falls [33].
The leading fall risk factor among the group of people who fell after the intervention was having a middle central neurological condition (such as stroke or Parkinson’s disease. Most previous studies assessing the effectiveness of geriatric comprehensive fall prevention clinics tend to exclude these patients, making our findings of a trend in reducing fall risk an interesting advance.
There was a trend towards featuring more cognitive disorders (33%) in patients who fell after the intervention, although no significant difference was found on the Folstein test [34]. According to several studies, older adults who fall perform worse in specific cognitive domains, such as attention [35,36]. Divided attention refers to the ability to carry out more than one task simultaneously and is required in most activities of daily living. A post-analysis record review revealed that most patients who experienced multiple falls six months after the intervention had cognitive or behavioral disorders. Indeed, our clinic’s design, which included a specialized interpretation of the cognitive assessments, would allow us to accurately identify those at higher risk of falls.
In our study, the primary intervention for patients who experienced more falls after the intervention was to schedule a medical follow-up. This indicates that the patients were accurately identified during the initial evaluation and were closely monitored to help promote their response to interventions. Finally, requests for a home visit by an occupational therapist were more frequent in patients with recurrent falls. This suggests that the team had identified a persistent functional problem and tried to ascertain the palliation of fixed deficits through a home visit with an occupational therapist.
At T1, the leading fall risk factors of patients who did not fall after the intervention were deconditioning, peripheral neurological disorder, and superior central neurological issues (potential dementia, pre-frontal ataxia). These patients were primarily directed to an exercise and mobility program (at home, at a day hospital, or in the community), they often had walking aids prescribed, and medication was adjusted. Based on these results, we hypothesize that using a multifactorial assessment, obtaining a precise diagnosis, and recommending targeted treatment strategies was appropriate. Since the majority of current Fall Prevention Clinics offer limited or standard assessments and treatment plans, our design may be more appropriately aligned with Tinetti’s recommendations [12]. The team, including a nurse, a physiotherapist, and a geriatrician, established rigorous complementary interdisciplinary work to target the leading causes of falls in participants. Within our Fall Prevention Clinic, the stepwise multidisciplinary evaluation of patients increased the number of kept appointments and improved the efficiency of assessment and intervention for all the professionals. In addition, the history of falls collected the day before the initial visit prepared the patients to accept a lengthy consultation relevant to their problem, while increasing their confidence in the process and the quality of their answers.
The same nurse monitored the occurrence of falls with the patients for the next six months and contributed to implementing the personalized intervention plan. Fall event recordings and follow-ups were important components of the program [37], as they allowed us to document delays before the start of the intervention aimed at improving strength, balance, and gait, as well as an occupational therapist’s visit.
LimitationsAlthough our study suggests that our Fall Prevention Clinic design helps reduce the risk of falls among a high-risk elderly population, it has several limitations. First, its design is a pre-post single-group longitudinal study without a blinded assessor; a prospective control-group study would offer greater certainty regarding the actual effect on fall rates and the number of subsequent falls. A multifactorial intervention can effectively reduce fall risks, although its clinical application depends on the timely availability of resources to address modifiable fall factors. Additionally, our intervention, such as physical activity, may vary among participants since there was no standardised exercise program guided by a manual, for example. Conversely, geriatric care was provided by all involved geriatricians following best evidence-based practices. A significant issue is that it was not always possible for patients to receive the targeted intervention within a reasonable timeframe and at the appropriate intensity. Allied health resources (physiotherapy, occupational therapy, etc.) in geriatrics are limited in our community and are mainly dispersed across various programs, which hampers the prioritisation of high-risk patients. Sometimes, several months would pass before our patients could begin the programs or access the resources to which they were referred.
Conversely, this study was conducted at a university-affiliated clinic, which may have access to more specialized professionals than smaller community hospitals. The reproducibility of such a setting would require a clinical nurse in geriatrics, a physiotherapist experienced in geriatrics and falls assessment, and geriatricians. Additionally, community resources for physical activities, such as falls prevention programs, might vary across centers. Nevertheless, high-risk and very high-risk fallers rely on several health resources. Our design of a fall prevention clinic in Quebec could be a more efficient way to allocate services that these patients would need to access anyway.
Additionally, due to our population’s frailty, we lost a significant part of our initial sample (only 50% completed the entire study). Due to attrition bias, the patients who finished the study might represent a healthier subset of the population. A larger sample size would provide greater power to determine which intervention is more effective. It could help identify which patients might benefit from specific interventions based on their diagnosed risk factors. Furthermore, the low annual incidence of falls likely reduced the study’s power. A limited budget and time constraints restricted the participant sample. Future studies could benefit from a larger sample size and longer follow-up periods to improve statistical power.
A future study should control its interventions: Promptness and intensity should be optimized for mobility and exercise programs. Management delays should be minimized, sufficient intensity ensured, and interventions should not rely solely on community services and existing rehabilitation facilities. We propose a second phase for our study: a randomized controlled trial (RCT) where participants follow our design of a Falls Prevention clinic. One group would be referred to the programs available through public and community services, while the intervention group would receive a tailored, in-house physical exercise program focused on balance, with controlled delays before initiation.
Following a single visit to our originally designed Fall Prevention Clinic, a targeted multifactorial fall prevention program trended toward reducing falls among high-risk older adults. Falls can be prevented when risk factors are accurately identified and appropriate interventions are implemented promptly. The management of falls by an interprofessional team within a Fall Prevention Clinic provides an opportunity to make medical and psychosocial diagnoses and to identify key modifiable risk factors.
The study received approval from the Ethics Committee of the Centre Intégré universitaire de Santé et de Services Sociaux de l’Estrie—Centre hospitalier universitaire de Sherbrooke (CIUSSS de l’Estrie—CHUS) (protocol 2018-2689, approved on May 25, 2018). Informed consent was obtained from all participants involved in the study.
Declaration of Helsinki STROBE Reporting GuidelineThis study adhered to the Helsinki Declaration, and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were followed.
The dataset for this study is available from the authors upon reasonable request.
SB, HC, JL, GR, EB designed the study. SB, JL, GR, EB collected data, and SB, HC, CP, EB analysed and interpreted the data. SB, HC, CP, EB drafted the manuscript, but all the authors provided critical revisions.
The authors declare that they have no competing interests.
This research was funded by the Vitae Foundation, Program 2017–2018.
We would like to thank the nurses and support staff of the Argyll Geriatric Ambulatory Clinics for their collaboration, as well as to the technical support team at the Research Centre on Aging (CDRV) for their assistance in providing technological resources that facilitated data collection. We also acknowledge the financial assistance rendered by the Vitae Foundation.
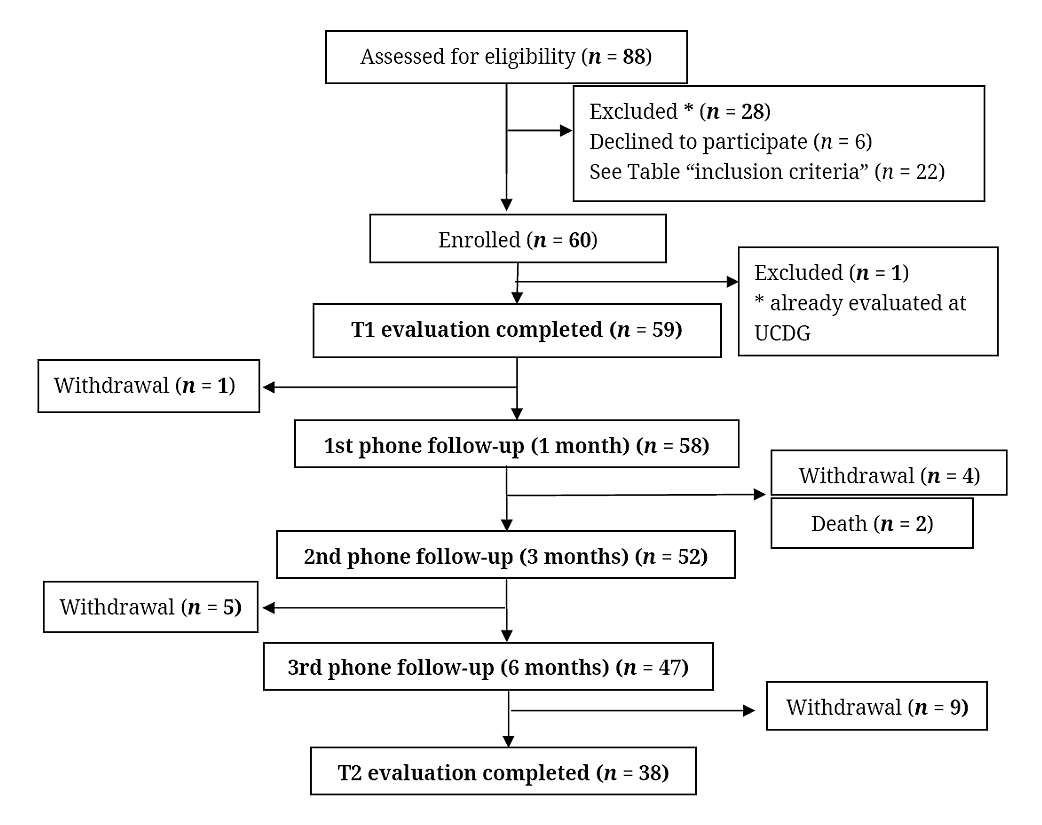
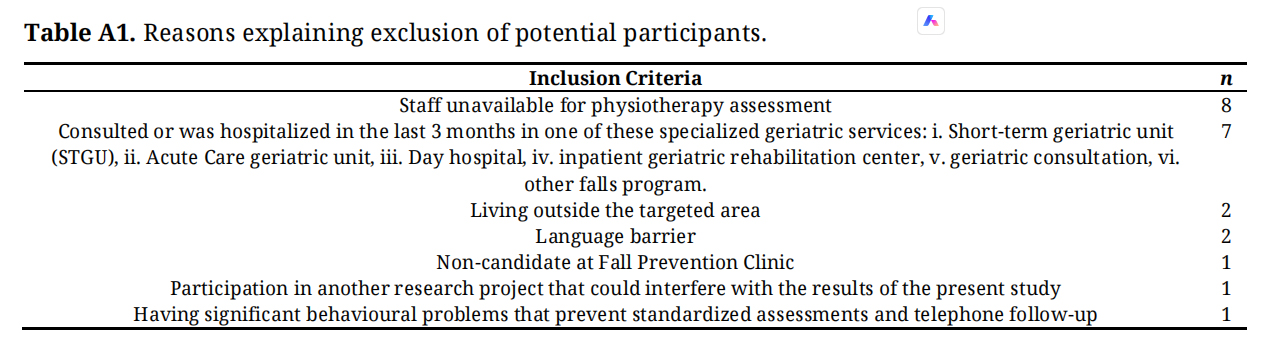 Table A1. Reasons explaining exclusion of potential participants.
Table A1. Reasons explaining exclusion of potential participants.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Brazeau S, Corriveau H, Lapierre J, Ricard G, Pagé C, Breton É. An interdisciplinary outpatient clinic designed to reduce falls in community-living seniors: A pragmatic pilot study. Adv Geriatr Med Res. 2025;7(4):e250022. https://doi.org/10.20900/agmr20250022.

Copyright © Hapres Co., Ltd. Privacy Policy | Terms and Conditions




